I was recently asked to review a cosmetic microneedling device white paper, meaning not a peer-review publications, rather an internal document generated by a company for sales purposes, from a company in Texas called Procell. As I’ve reported previously in peer-reviewed, PubMed listed papers, microneedling is a deep wounding procedure that activates the innate and adaptive immune systems and induces a wounded-proliferative state in the skin that is inflammatory and possibly pro-oncogenic. Sadly, this company, with its medical director (Mitchel Schwartz), who has no peer-reviewed publications and is paying for this study, is selling this product online and apparently making illegal sales to estheticians in states where microneedling procedures performed on others by estheticians is illegal.
The study in question here was performed by a physician in Canada who has no peer-reviewed publications, and the study, and the physician performing the study, were paid by Procell. The Procell device uses an array of needles that are 250 micrometers in length, with the thickness of the needles not reported. The device is run over the face such that these needles are puncturing holes in the epidermis and dermis at high rates, thus injuring both the epidermis and dermis.
The study design and the results are indicative of an inexperienced practitioner performing a study. First, the author states, “This study is a prospective, evaluator-blinded, single-site study, involving up to 30
subjects comparing clinical benefits after a treatment series versus baseline.” The claim of “evaluator-blinded” is ridiculous. Each subject serves as her own control, with photos being taken before and after treatment, and its easy for the evaluator to know who they are analyzing. Then they have a section called, “3.5 Randomization of Subjects.’ There is no randomization of the subjects. All are given the treatment. Next they say that “Photographic assessments will be conducted by a blinded expect evaluator.” I think they meant “expert” instead of “expect.” Although I think “expect evaluator” is the better descriptor, I’ll give them the benefit of the doubt. Regardless, the evaluator can easily identify each patient through their photos, and know what picture has been captured before and after the procedure. This is all just gobbledygook, and is either a consequence of ineptitude and/or fraud.
There are no results presented in the paper, only a conclusion. Yes, that’s right. No results are presented. What they do present in their “Safety Analysis” is a set on incongruous statements about how one patient was injured. Here’s what they reported in their “Safety Analysis”:
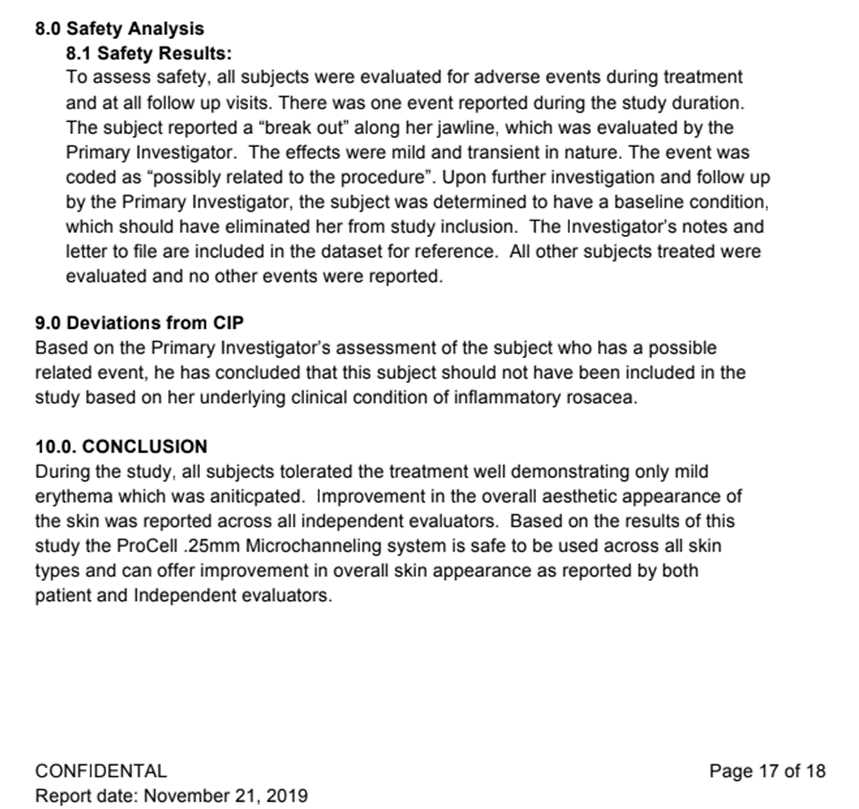
8.0 Safety Analysis
8.1 Safety Results:
To assess safety, all subjects were evaluated for adverse events during treatment and at all follow up visits. There was one event reported during the study duration.
The subject reported a “break out” along her jawline, which was evaluated by the
Primary Investigator. The effects were mild and transient in nature. The event was
coded as “possibly related to the procedure”. Upon further investigation and follow up
by the Primary Investigator, the subject was determined to have a baseline condition,
which should have eliminated her from study inclusion. The Investigator’s notes and
letter to file are included in the dataset for reference. All other subjects treated were
evaluated and no other events were reported.
My comment: (here they’re saying one of the patients had an adverse reaction)
9.0 Deviations from CIP
Based on the Primary Investigator’s assessment of the subject who has a possible
related event, he has concluded that this subject should not have been included in the
study based on her underlying clinical condition of inflammatory rosacea.
My comment: (here they’re saying the physician screwed up and shouldn’t have included this patient in the study)
10.0. CONCLUSION
During the study, all subjects tolerated the treatment well demonstrating only mild
erythema which was aniticpated [sic]. Improvement in the overall aesthetic appearance of
the skin was reported across all independent evaluators. Based on the results of this
study the ProCell .25mm Microchanneling system is safe to be used across all skin
types and can offer improvement in overall skin appearance as reported by both
patient and Independent evaluators.
My Comment: (here they contradict themselves, saying that the procedure is good for all skin types)
Here’s an image from the study so you can see for yourself:
Combine this inflammatory-proliferative, injurious procedure with the bone marrow mesenchymal stem cell cytokines that they sell, and one has set themselves up for adverse events, possibly long-term. There are skin conditions for which microneedling, when not performed repeatedly, is beneficial and the benefits out way the risks. Acne scarring and other types of scars can be an example. To quell the inflammation associated with the procedure and to set the immune system into a anti-inflammatory, pro-repair state, use the S2RM technology, found to be safe and efficacious, contained in Neogenesis Recovery.




