Despite the years of research on the ill effects of SLS (sodium lauryl sulfate), I continue to hear that people, including dermatologists, are using products with this ingredient, including shampoos.
If you’ve ever Googled the causes of a skin irritation or damaged hair, you’ve likely seen posts about SLS, or sodium lauryl (or laureth) sulfate, a common ingredient in beauty products, cleansers, shampoos, toothpastes, and cleaning products.
So what does this ingredient do, why is it in everything, and what does the evidence say about how safe it is?
When we use a cleanser or shampoo, the product usually contains a detergent. That detergent is called a surfactant. A surfactant allows the oil and water molecules to bind together – it’s what’s found in soaps and detergents so we can wash our oily faces or dishes with water and remove the grime.
Sodium lauryl sulfate (SLS) is a surfactant, and its efficacy, low cost, abundance and simplicity mean it’s used in a variety of cosmetic, dermatological, and consumer products.
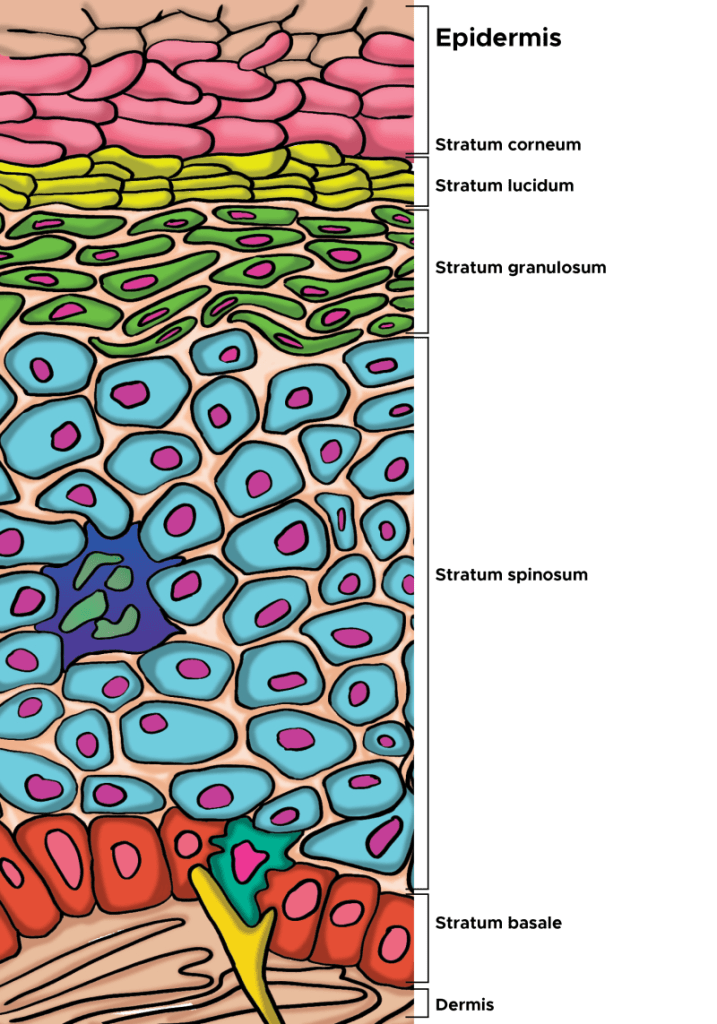
Our skin’s outermost layer, the stratum corneum of the epidermis, is specially designed to keep harmful things out, and this is where a surfactant can cause problems. Using chemicals that weaken this barrier defence mechanism can potentially cause our skin harm.
As the outermost layer of the epidermis, the stratum corneum is the first line of defense for the body, serving an essential role as a protective skin barrier against the external environment. The stratum corneum aids in hydration and water retention, which prevents skin cracking, and is made up of corneocytes, which are anucleated keratinocytes that have reached the final stage of keratinocyte differentiation(From Murphrey et al, 2022).
Some surfactants are more irritating to our skin than others. For something to be harmful, irritating or allergenic, it has to fulfill two criteria. It has to have been found in studies to irritate human skin, and it has to have the ability to penetrate the skin. SLS does both. It penetrates the stratum corneum and induces an immune reaction, and degrades the structure of the barrier.
Scientists in Germany tested 1,600 patients for SLS irritancy and found 42% of the patients tested had an irritant reaction. Another study, on seven volunteers over a three and a half month period, found regular contact caused irritation, and the irritation subsided once the skin was no longer exposed to SLS. Another study found the warmer the water used with SLS, the more irritating it will be.
SLS is a well established irritatant and is used as a positive control in dermatological testing. That is, new products being tested to see how irritating they might be to human skin are compared to the known irritant, SLS. If a person is sensitive to SLS, they might find the area that has been in contact is red, dry, scaly, itchy or sore. It’s also important to note there’s no scientific evidence SLS causes cancer, despite what is often posted on the internet. So, it’s probably OK to use SLS in products that are used for household cleaners.
Who should avoid SLS?
Everyone, especially people with a history of sensitive skin, hyperirritable skin and patients suffering from skin conditions such as atopic dermatitis (eczema), rosacea, and psoriasis are best to avoid products containing SLS. If you think it might be SLS causing a skin irritation, stop the use of the product and look for products that don’t contain SLS.
The modern world’s dramatic increase in the number and types of chemicals in which man is exposed, a major part of of someone’s exposome, responsible for about 90% of diseases (not genetics), is causing a dramatic rise in noncommunicable and communicable diseases. Over 350 000 chemicals and mixtures of chemicals have been registered for production and use, up to three times as many as previously estimated, and an underestimate of the true number of chemical types that have been produced and commercialized. As the skin and other epithelial tissues are compromised and exposed to communicable diseases, skin and epithelial transmitted diseases are on the rise. For example, the shingles virus can enter through the skin or the epithelial tissue in our respiratory tract, and having shingles can even lead to increased risk of dementia(2nd Ref). Further, a compromised skin epithelial barrier caused by environmental factors such as mechanical trauma, exposure to exogenous proteases in microorganisms and our food, detergents, and air pollution can activate the innate and adaptive immune systems, inducing keratinocytes to release pro-inflammatory cytokines and chemokines and enhancing the antigen presentation by intradermal Langerhans cells (LCs) and dermal DCs and activating T-cells. In turn, for example, activation of T2 type T-cells leads to IL-4, IL-5, and IL-13 secretion, provoking skin barrier alteration, immune cell infiltration into skin, and itch as observed in atopic dermatitis.
The first essential step to skin immunity is the epithelial barrier, as infection and resulting inflammation are impossible without first breaching it. Epithelia, coated with a sugary glycocalyx, not only comprise our skin but also the mucosal membranes that line our organs. Their ability to secrete squalene, mucus, lipids, and antimicrobials help protect against pathogen invasion. Additionally, epithelia can prevent inflammation by physically shoving out cells infested with toxins, allergens, antigens, pathogens, or other damage by seamlessly extruding them. This is a strategy employed by not only epithelia, but also our hair does the same as it sheds. Given that chronic inflammation could stem from a defective epithelial barrier, the current approach of treating only the inflammation will only partially mitigate symptoms of a more central problem, ongoing wound healing and disrupted barrier.
Scientists now understand that in patients with allergic disease, regardless of tissue location, the homeostatic balance of the epithelial tissue barrier is skewed toward loss of differentiation, reduced junctional integrity, and impaired innate defense and a hyperactive adaptive (trained immunity) immune system. Importantly, epithelial dysfunction characterized by these traits appears to pre-date a predisposition to immunological responses against a range of antigens or allergens, and development of allergic disease.
From the disease perspective, trained immunity is beneficial, as it improves the host’s defense against subsequent infection from pathogens. However, it can also be detrimental and result in overly active immune responses or chronic inflammation. Even the innate immune system has some memory, given evidence that components in House Dust Mite extract activate and likely train macrophages to produce high amounts of CCL17, IL-6, and cysteinyl leukotrienes following re-exposure to HDM through the TNF-α and PGE2 pathways. Thus, an activated immune system, one that has memory and is primed to react, can lead to sensitivities that may be triggered by an overabundance of chemicals in the environment, and those sensitivities heightened by a disrupted barrier.
Evidence that epithelial barrier dysfunction explains the growing prevalence and exacerbations of inflammatory diseases such as eczema has grown through many studies performed world-wide. Diseases encompassed by the epithelial barrier theory share common features such as an increased prevalence after the 1960s that cannot be accounted soley by the emergence of improved diagnostic methods. They are indeed increasing in prevalence, i.e. the number of afflictions per 1,000 people.
Eepithelial barrier dysfunction enables the microbiome’s translocation from the skin’s surface to interepithelial and deeper subepithelial areas, doing in combination with allergens, toxins, pathogens, and pollutants. Thereafter, microbial dysbiosis and possible infection, characterized by colonization of opportunistic pathogenic bacteria and loss of the number and biodiversity of commensal bacteria results. Local inflammation, impaired tissue regeneration, and remodeling characterize the skin that suffers from impaired barrier. For example, commensal bacteria on the skin’s surface are important for epidermal lipid synthesis and improve barrier function. The skin’s microbiome is therefore critical to maintaining epidermal barrier function. The infiltration of inflammatory cells and inflammatory cytokines to affected tissues is part of the immune system’s response to erradicate invading bacteria, allergens, toxins, and pollutants away from the deep tissues. As Peter Elias, M.D. has written, “AD [atopic dermatitis] can be considered a disease of primary barrier failure, characterized by both a defective permeability (Proksch et al., 2006, and references therein) and antimicrobial function.” Further, inflammatory cells and inflammatory cytokines that migrate from the skin to other organs may play roles in the exacerbation of various inflammatory diseases in other organs. Thus, inflammation iniated in the skin may contribute to chronic inflammatory diseases in other tissues.
What Dr. Elias has been saying is that the permeability-barrier abnormality in AD is not merely an epiphenomenon but rather the “driver” of disease activity, an “outside–inside view of disease pathogenesis” (Elias and Feingold, 2001). The evidence for this is: (1) the extent of the permeability-barrier abnormality parallels severity of disease phenotype in AD, (2) both clinically uninvolved skin sites and skin cleared of inflammation for as long as 5 years continue to display significant barrier abnormalities, (3) topical artificial barrier therapy comprises effective ancillary therapy, and (4) specific replacement therapy, which targets the prominent lipid abnormalities that account for the barrier abnormality in AD, not only corrects the permeability-barrier abnormality but also comprises effective anti-inflammatory therapy for AD (Figure 1; Chamlin et al., 2002). Thus, inflammation in AD may begin with insults from without, i.e. the exposome.
That barrier insult can then activate epithelial cells in the skin, keratinocyes, which are non-professional immune cells, but do possess MHC-II molecules, that present antigens to professional immune cells, such as T-cells. Thus, with disrupted barriier, the keratinocytes can recognize antigens and present them to the immune system, leading to inflammation. More and more, scientists are discovering how epithelial cells are part of the immune system, regardless in which organ they exist. Key here is to protect barrier function in all of our epithelial tissues, including the skin.
So if inflammatory diseases such as eczema and psoriasis are environmentally triggered and lead to barrier dysfunction and resultant inflammation, what can we do?
Second, use a topical product that provides the 3 lipids and natural moisturizing factors that are needed to rebuild normal stratum corneum and barrier function. One product to use is NeoGenesis Barrier Renewal Cream (BRC).
Third, use a product that provides instantaneous barrier function and commensal bacteria. The instantaneous barrier allows the BRC to rebuld the natural barrier function over time, and the commensal bacteria help to rebuild the barrier through activation of lipid synthesis by skin cells. The commensal bacteria in Neogenesis MB-2 also help to reduce the Staphylococcus aureus infection often assicated with disrupted barrier function.
So remember, these inflammatory skin conditions are triggered by the environment. Therefore, their treatment and prevention means that if you change your environment, you can prevent or treat these diseases. Part of changing your environment is the careful choice of topical products to reduce inflammation and renormalize the structure and function of your skin.
Psoriasis is a relapsing–remitting immune-mediated skin disorder characterized by epidermal overgrowth, and massive inflammatory infiltrates as hallmarks of scaly erythematous lesions. Epigenetic changes detected in epidermal keratinocytes of resolved skin may be responsible for the DRTP (disease-residual transcriptomic profile) in the same regions, leading to a reoccurrence of the lesion. I’ll explain some ways, including new technologies for epigenetic regulation, to better treat psoriasis.
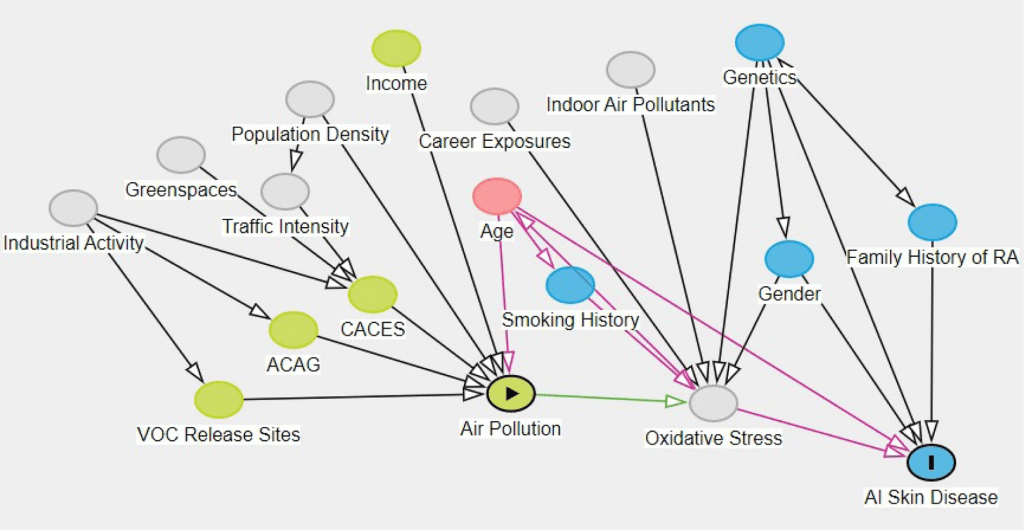
The multifactorial causes of inflammatory skin conditions, including psoriasis. From: Lowe et al (2022)
Like most diseases, psoriasis is environmentally triggered. You can think of it as mismatch between hereditary factors, including but not just genetics (Bonduriansky, 2012), and the environment. The modern environment is full of triggers for psoriasis, such as air and water pollution (Lowe et al, 2023) and poor diets (Kanda et al, 2020), and our hereditary factors have not adapted to the new environment. With over 2,000 new chemicals introduced into the USA each year, genetic based heredity will never adapt us to our ever changing environment. Evolutionary adaptation based on genetics requires too much time, usually at least thousands of years. For example, the recent introduction of eating processed food with high amounts of salt (sodium) can lead to sodium accumulation in the skin, and can be an inflammatory factor in psoriasis (Maifeld A et al, 2022), dramatically impeding skin remodeling (Pajtók et al, 2021). People haven’t yet adapted to high levels of dietary sodium, and so it is causative, at least partially, in many diseases (Lucarini et al, 2021), including psoriasis.
An example of the slow genetic hereditary adaption to the environment is lactose tolerance in some populations of humans where the environment included cattle and the milk they made available to humans. Studies of DNA from 40,000 years ago up to a few hundred years ago show that there has been a very rapid rise of the genetic variant that helps humans consume milk as adults, called lactose tolerance. The genetic variant didn’t become common until the past 1,000 to 2,000 years. With thousands of years of heredity, humans who co-evolved with cattle developed the ability to drink the milk of cattle. In East Asia, where cattle were not common, the people remained lactose intolerant (Goh et al, 2018).
However, and important to disease states such as psoriasis (Dopytalska et al, 2021), epigenetics, another hereditary factor that is not genetic, can play significant and rapid roles in adaptation to the environment (Carneiro et al, 2020). Epigenetics is not changes in the DNA itself, rather it is environmentally triggered changes in the expression of DNA. In other words, epigenetics is about what DNA is turned-on or turned-off by environmental factors. These genetic and epigenetic adaptations can turn out to be maladaptive given the rapid and ever changing environment in today’s modern world. That is, you epigenetically adapt to one thing in the environment, but another thing comes along in the environment that is a mismatch for the epigenetic adaption. That epigenetic maladaptation can pass on to your offspring and their offspring (Fitz-James and Cavalli, 2022). But there is good news. Scientists in Germany have demonstrated that maladaptive epigenetics in human skin can be reversed to some degree by using naturally sourced DNA methylation inhibitors , leading to better skin health (Falckenhayn et al, 2024). Methylation is one of the key means by which DNA can be turned-on of turned-off.
Considering psoriasis, like most bodily functions, epidermal desquamation is a highly regulated process of corneocytes shedding from the outermost layers of the stratum corneum (Haftek, 2015). Psoriasis is a condition where skin cells replicate at an abnormally fast rate. This leads to a buildup of dead, interconnected skin cells on the surface, forming the thick, silvery plaques and a lack of moisture that characterize this condition. Normal shedding of corneocytes is disrupted, leaving a thick patch of dried skin tissue.
So let’s look at how we can renormalize the physiology of psoriatic skin using three key topical products currently on the market, and one that will be released soon.
Salicylic acid (SA)
Salicylic acid (SA) is a keratolytic that promotes stratum corneum desquamation (Elmets et al, 2021). Evidence suggests that SA works by digesting skin keratin and disrupting barriers to water-binding functions that allows the skin plaques to desquamate (Rawlings et al, 1994). Like the enzymes involved in filaggrin degradation, the hydrolases (enzymes that depend on water to breakdown the structures) involved in desmosome degradation and lipid degradation are dependent upon water for their activity. However, water activity within the stratum corneum is dependent upon the NMF and lipids. When adversely influenced by many factors, such as degraded barrier function, insufficient stratum corneum moisturization and water content leads to defective desquamation.
SA works best when an occlusive and moisturizing formulation is applied on top of the salicylic acid gel, thereby creating an environment optimal for barrier repair, where moisture is retained, thus maximizing normal enzyme activity and minimizing the irritating effects of SA.
At Neogenesis, we use an OTC drug form of SA that contains 2% salicylic acid. This is a mild form of SA and can be used daily for moderate to severe forms of psoriasis. Stronger forms of salicylic acid, which have side effects, are available by prescription from your dermatologist. As for all drugs, follow the OTC label on all salicylic acid products before applying.
2. Moisturizers
Considering the NMF and lipids that are important for treating psoriasis, NeoGenesis’ Barrier Renewal Cream (BRC) features NMF and lipid ingredients critical to barrier repair and remediating psoriasis. These ingredients include, Urea, Squalane, Caprylic/Capric Triglyceride, Safflower Oleosomes, Glycerin, Sodium PCA, Ceramide NP, Ceramide AP, Ceramide EOP, Phytosphingosine, Cholesterol, and Sodium Hyaluronate Butyrate. Not only is BRC providing necessary lipids and NMF to rebuild the epidermal barrier, but butyrate is another key molecule for epidermis. Butyrate, originating from gut bacteria and skin bacteria, has been found to increase Treg and reduce inflammation in the skin (Schwarz et al, 2017), regulate mitochondrial function of keratinocytes (Trompette et al, 2022) and to increase the expression of FLG protein by inhibiting the activity of histone deacetylase, and restoring the function and permeability of the epidermal barrier (Kleuskens et al., 2022).
3. S2RM – Stem Cell Released Molecules
The molecules in S2RM inhibit the proliferation of activated T cells, modulate the release of inflammatory cytokines and chemokines by dendritic cells and macrophages, suppress proliferation and immunoglobulin production of B cells, and inhibit cytotoxic activity of natural killer (NK) cells. The positive effects of topically applied stem cell released molecules in psoriasis are dramatic and occur quickly (Seetharaman et al, 2019). Controlling all of these functions in psoriatic skin using S2RM is highly important to controlling inflammation and autoimmunity.
4. Something New – Autoimmune, DNA Methylation Modulators
Epigenetic mechanisms of gene expression regulation are a group of the key cellular and molecular pathways that lead to inherited alterations in genes’ activity without changing their DNA coding sequence. Methylation of cytosine residues in the CpG island located in the gene promoter region of DNA causes suppression of gene expression, while these unmethylated regions of DNA leads to activation of gene expression. Modulation of methylation can therefore turn on or turn off gene expression and in this way remove or modify epigenetic “memories.” In this way, if the cells of the skin have an epigenetic memory of a chronic inflammatory event, for example, epigenetic modulators can eliminate or reduce this memory.
I won’t go into details here, but many long coding RNAs are involved in the immunopathogenesis of psoriasis (Tsoi LC et al, 2015), and long non-coding RNA (lncRNA) mediates DNA methylation in both physiological and pathological conditions (Huang et al, 2022). A lncRNA named PRINS (Psoriasis susceptibility-related RNA Gene Induced by Stress) has been found to be essential in the survival of keratinocytes under stress condition and is thought to contribute to psoriasis susceptibility (Sonkoly et al, 2005). Epigenetic changes detected in epidermal keratinocytes of resolved skin may be responsible for the DRTP (disease-residual transcriptomic profile) in the same regions, leading to a reoccurrence of the lesion (Ghaffarinia et al, 2023) . If the epigenetic changes in keratinocytes can be erased, then the reoccurrence of the psoriatic lesions may be abated.
Falckenhayn et al (2024) found that natural, plant-based DNA methylation inhibitors were able to penetrate the skin. For example, they found dihydromyricetin, which (for you chem nerds) has a molecular weight of 320.25 g/mol and a logP of 1.23 (ChemSpider) was able to penetrate into living skin cells. The positive effects they found included increased epidermal thickness and a more youthful set of cellular parameters. As a result, fewer wrinkles (3.7 tears of wrinkle accumulation were removed) were found in treated skin compared to controls. Other natural ingredients, including cannabinoids have been found to modulate DNA methylation and reduce skin autoimmunity and inflammation.
Cannabinoids are of great interest to me because I personally know the power of the endogenous cannabinoid systems in the body. When I was professor at UCSD, my lab discovered the cannabinoid signaling system in the eye, and later found with colleagues at UCSB that when the endogenous cannabinoid system is fully activated, neurons, called retinal ganglion cells, are protected from neurodegeneration. It is indeed, a very powerful system throughout the body involved in immune function and epigenetics.
For example, the first evidence describing the possible effects of CBD and CBG on DNA methylation aimed at clarifying the epigenetic regulation of keratinocyte differentiation by phytocannabinoids. Their study used human kHaCaT cells, revealing that CBD increased global DNA methylation and decreased gene expression involved in keratinocyte differentiation. In other words, CBD and CBG slowed down replication of keratinocytes. Again, psoriasis is characterized by an excessive proliferation and abnormal differentiation of keratinocytes and infiltration of multiple inflammatory cells. Interestingly, CBD effects on DNA methylation and gene expression were mimicked by AEA and blocked by a selective CB1 antagonist, suggesting an indirect mechanism rather than a direct regulation by CBD (Pucci et al, 2013). Many people haven’t heard about the power of CBG, but it is a very powerful antioxidant and anti-inflammatory in the skin (Perez et al, 2022).
I’ll tell you more about it later, but we currently have a product in testing that features a number of phytochemicals, including CBD and CBG and other epigenetic modulators. It’s sure to help a number of inflammatory skin conditions, including psoriasis. Stay tuned.
References
Bonduriansky R. (2012) Rethinking heredity, again. Trends Ecol Evol. 27(6):330-6
Carneiro VC et al (2020) Rapid Epigenetic Adaptation in Animals and Its Role in Invasiveness, Integrative and Comparative Biology, Volume 60, Issue 2, Pages 267–274,
Dopytalska K, Ciechanowicz P, Wiszniewski K, Szymańska E, Walecka I. The Role of Epigenetic Factors in Psoriasis. Int J Mol Sci. 2021 Aug 27;22(17):9294.
Elmets CA et al. (2021) Joint AAD-NPF Guidelines of care for the management and treatment of psoriasis with topical therapy and alternative medicine modalities for psoriasis severity measures. J Am Acad Dermatol. 84(2):432–470.
Falckenhayn C et al (2024) Identification of dihydromyricetin as a natural DNA methylation inhibitor with rejuvenating activity in human skin. Front Aging. 4:1258184.
Fitz-James, M.H., Cavalli, G. (2022) Molecular mechanisms of transgenerational epigenetic inheritance. Nat Rev Genet23, 325–341.
Ghaffarinia A et al (2023) Psoriatic Resolved Skin Epidermal Keratinocytes Retain Disease-Residual Transcriptomic and Epigenomic Profiles. Int J Mol Sci. 24(5):4556
Goh LH et al (2018) Lactase deficiency and lactose intolerance in a multiracial Asian population in Malaysia. JGH Open ;2(6):307-310.
Haftek M. Epidermal barrier disorders and corneodesmosome defects. Cell Tissue Res. 2015 Jun;360(3):483-90.
Huang, W., Li, H., Yu, Q. et al. (2022) LncRNA-mediated DNA methylation: an emerging mechanism in cancer and beyond. J Exp Clin Cancer Res41, 100.
Kanda N, Hoashi T, Saeki H. Nutrition and Psoriasis. Int J Mol Sci. 2020 Jul 29;21(15):5405.
Lowe, M.E et al (2023) The skin is no barrier to mixtures: Air pollutant mixtures and reported psoriasis or eczema in the Personalized Environment and Genes Study (PEGS). J Expo Sci Environ Epidemiol 33, 474–481.
Lucarini M et al (2021) Sodium Intake and Related Diseases. Int J Mol Sci. 22(14):7608
Maifeld A et al (2022) Skin Sodium Accumulates in Psoriasis and Reflects Disease Severity. J Invest Dermatol. 142(1):166-178.e8.
Pajtók C, Veres-Székely A, Agócs R, Szebeni B, Dobosy P, Németh I, Veréb Z, Kemény L, Szabó AJ, Vannay Á, Tulassay T, Pap D. (2021) High salt diet impairs dermal tissue remodeling in a mouse model of IMQ induced dermatitis. PLoS One. 16(11):e0258502.
Perez E, Fernandez JR, Fitzgerald C, Rouzard K, Tamura M, Savile C. (2022) In Vitro and Clinical Evaluation of Cannabigerol (CBG) Produced via Yeast Biosynthesis: A Cannabinoid with a Broad Range of Anti-Inflammatory and Skin Health-Boosting Properties. Molecules. 27(2):491.
Pucci M et al (2013) Epigenetic control of skin differentiation genes by phytocannabinoids. Br J Pharmacol. 170(3):581-91.
Schwarz A, Bruhs A, Schwarz T (2017) The Short-Chain Fatty Acid Sodium Butyrate Functions as a Regulator of the Skin Immune System. J Invest Dermatol. 137(4):855-864.
Seetharaman R et al (2019) Mesenchymal Stem Cell Conditioned Media Ameliorate Psoriasis Vulgaris: A Case Study. Case Reports in Dermatological Medicine. Volume 2019 | Article ID 8309103.
Sonkoly E et al (2005) Identification and characterization of a novel, psoriasis susceptibility-related noncoding RNA gene, PRINS. J Biol Chem. 280(25):24159-67.
Trompette, A., Pernot, J., Perdijk, O. et al. (2022) Gut-derived short-chain fatty acids modulate skin barrier integrity by promoting keratinocyte metabolism and differentiation. Mucosal Immunol15, 908–926.
Tsoi LC et al (2015) Analysis of long non-coding RNAs highlights tissue-specific expression patterns and epigenetic profiles in normal and psoriatic skin. Genome Biol. 16(1):24.
Activation of the aryl hydrocarbon receptor (AhR) through its natural ligands, has been found to reduce skin inflammation, reduce oxidative stress, and upregulate skin barrier protein expression. AhR also inhibits the generation, persistence, and cytokine production of resident memory T cells in the skin. Stem cell released molecules (secretome) from adipose mesenchymal stem cells includes kynurenine, which is an AhR agonist.
The molecules released (secretome) from adipose mesenchymal stem cells (ADSCs) are diverse (Maguire, 2013) and and have many immunotherapeutic actions. Recent studies provide evidence that one mechanism by which the secretome of ADSCs act is through their agonist activities at Aryl hydrocarbon receptors (AhR). Such AhR agonist activity is highly therapeutic to eczema (Eichenfield et al, 2023).
The aryl hydrocarbon receptor (AhR) is expressed in various tissues characterized by a rapid growth rate, including human skin. Kynurenic acid, a product of tryptophan metabolism enzymatically formed from kynurenine, is a natural ligand for AhR. However, AhR is a promiscuous receptor, binding many unnatural ligands such as environmental toxins. This is important, because if the AhR is activated by unnatural ligands, such as air pollution (PM2.5 for example), ill effects can result. The soluble factors (kynurenine and downstream metabolites) generated by IDO (Indoleamine 2,3-dioxygenase) can bind and activate the aryl hydrocarbon receptor to promote Treg cell differentiation and the induction of dendritic cells expressing an immunosuppressive phenotype. Further, in a dose-dependent response, kynurenine upregulates the expression of immunosuppressive genes, such as TGFB1 and IDO1.
Mechanistically, ADSCs release kynurenine, which is a tryptophan metabolite catalyzed by IDO, to activate the aryl hydrocarbon receptor and enhance its downstream target NFE2L2 in macrophages. NFE2L2-encoded NRF2 not only functions as a master regulator of antioxidant defense but also represses the expression of inflammatory genes. As expected, NRF2 upregulation in macrophages was inhibited by inhibiting IDO and 1-methyltryptophan (1-MT), and the anti-inflammatory effect of ADSCs on macrophages was blocked when NRF2 expression in macrophages was silenced. Kynurenic acid, another IDO-derived metabolite that shares the same aryl hydrocarbon receptor as kynurenine, can promote TNF-α-stimulated gene-6 (TSG-6) expression, which is also released from ADSCs, and alleviate neutrophil infiltration of tissues (Wang et al, 2018).
In summary, the secretome from ADSCs contains a number of molecules (IDO, kynurenine, kynurenic acid) that naturally activate aryl hydrocarbon receptors to reduce inflammation in the skin, and provide long term therapeutic benefit to skin diseases such as Eczema and Psoriasis.
In a recent trial (Gupta et al, 2023), the blood pressure–lowering effect of dietary sodium reduction was comparable with a commonly used first-line antihypertensive medication. Salt in the diet is associated with chronic kidney disease. Sodium also accumulates in the skin, inducing inflammation and eczema, so feel better and look better by cutting the sodium intake that is way too high in most people.
Many factors can influence health, including that of the skin. I’ll discuss salt here, but other factors such as dairy play a big role too – both for cardiovascular health, and skin health. For example, the induction of antibodies (IgE) by the consumption of dairy can lead to cardiovascular disease and death. And dairy, loaded with antigens such as lactose, whey, and casein (even found in mothers milk because of dairy consumption by mom) can be destructive to the skin, even causing cancer.
As Gupta et al (2023) discovered, dietary sodium reduction significantly lowered blood pressure (BP) in the majority of middle-aged to elderly adults they studied. The decline in BP of those who went from a high- to low-sodium diet was independent of hypertension status and antihypertensive medication use, and was consistent across subgroups. Needless to say, reducing sodium intake did not result in adverse events.
Sodium is an essential mineral and osmolyte for the human body. It is the major cation in the extracellular fluid and as such plays a crucial role in homeostatic processes such as regulation of blood volume, osmolarity, and blood pressure. Therefore, sodium plasma concentration is maintained within a relatively narrow range of around 140 mmol/l. The sodium concentration in the interstitial space (the space in between our cells) can be much higher. We consume just the right amount of sodium when we eat a plant based diet without added sodium. If we eat too much sodium, that excessive salt intake may induce several adverse effects, causing microvascular endothelial inflammation, anatomical remodeling, and functional abnormalities, even in normotensive subjects (those with normal blood pressure). More recent studies have shown that changes in sodium plasma levels not only exert their effects on small resistance arteries, but may also affect the function and structure of large elastic arteries. The issue of salt-sensitivity, which refers to individual susceptibility in terms of BP variations following changes in dietary salt intake, has also been recently debated in its pathophysiological mechanisms and clinical implications.
Excess sodium is also stored in the skin. In the skin microenvironment, higher sodium concentrations enhance macrophage function, potentially leading to innate immune system-based inflammation. Several studies have provided significant evidence that an elevated sodium concentration has an immunomodulating effect by augmenting proinflammatory and antimicrobial macrophage function as well as T-cell activation. And now we know that sodium has accumulated to high levels in the skin of psoriasis patients (Maifeld et al, 2021). Psoriasis is an inflammatory skin condition, and restricting salt in your diet will help to reduce that inflammation. Same for eczema. Reduce the salt because, for one factor, salt promotes the growth of a bad bacteria called staph aureus which is found in patients who have bad flare ups of eczema. With high salt, the skin is unable to repair itself – it’s in a constant state of inflammation.
Cut the salt and your immune system will operate more normally. It requires time to adjust your taste to the low sodium diet – most of us are addicted to salt. But in time, you lose the addiction, and actually begin to better taste all of the other flavors in your food that were masked by the salt. Bon appetite, Pas de sel!