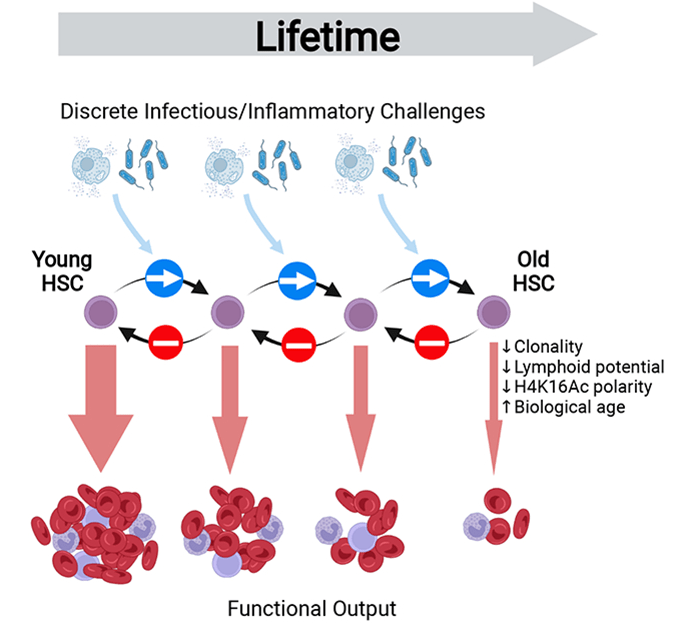
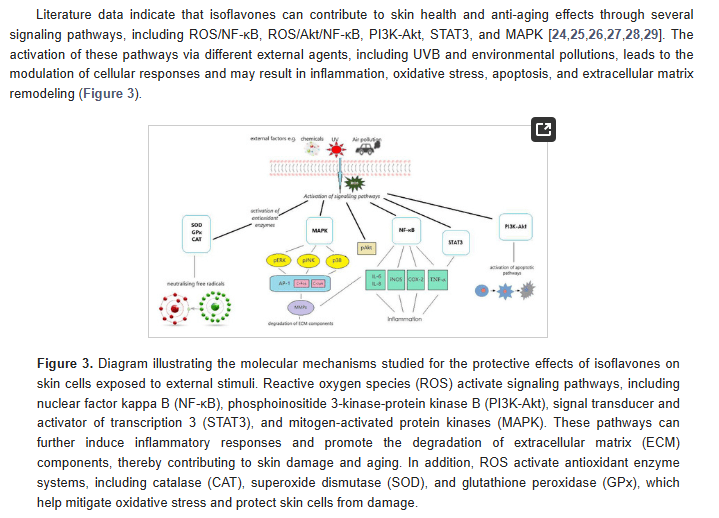
Early and mid-life inflammation ia a mediator of lifelong defects in tissue maintenance and regeneration due to the inflammation aging the stem cells.Inflammation damages the extracellular matrix, DNA, and epigenetic mechanisms, all of which contribute to aging and age-related diseases.
A schematic of stem cell inflammaging (from Bogeska et al, 2022)
Inflammaging, defined as an age-related increase in the levels of pro-inflammatory markers in blood and tissues, is a strong risk factor for multiple diseases that are highly prevalent, and frequent causes of disabilities in elderly individuals but are pathophysiologically uncorrelated, i.e., everything from cancer, to skin diseases, to heart disease, and neurodegeneration. And remember, as I’ve discussed in previous blogs, inflammation in the skin can can lead to systemic inflammation.
Inflammation can wreak havoc on the body, including the skin, through a number of key mechanisms. Let’s have a look at how inflammation can damage tissue, such as by degrading the extracellular matrix, and can damage cells at the molecular level through genetic and epigenetic mechanisms. Genetic refers to how damage occurs to the DNA, and epigenetic refers to how damage occurs “above” the DNA, such as the mechanisms that control the expression of DNA – i.e., affecting how the DNA makes RNA and proteins. Inflammation can also cause misfolding in proteins, resulting in a number of dysfunctional pathways in the body, including the control of epigenetics such as protein-based epigenetics. You read that right – proteins can be inherited and dysfunctional proteins in an adult can be inherited as dysfunctional proteins in the offspring. That’s one reason why genetics and heredity don’t mean the same thing.
Inflammaging is a process induced by chronic inflammatory cytokine signaling that promotes accelerated damage to the extracellular matrix (ECM), stem-cell aging, and precancer stem-cell generation. Multiple different sterile and infection-associated inflammatory stimuli have been shown to provoke primitive stem cells (HSCs) to exit their long-term quiescent state and enter into active proliferation. In other words, inflammation, whether it is sterile inflammation or infection-related inflammation, drives stem cells into a state where they multiply. Therefore, chronic inflammation will induce the constant multiplication of stem cells. And every time a cell multiplies itself, mutations and consequent aging processes will occur. As I’ve said before, one of the most dangerous things a cell can do is to multiply itself.
As scientists have recently published, their work demonstrates that inflammatory stimuli can provoke a long-lasting inhibitory effect on tissue regeneration that extends far beyond the duration of the original inflammatory event, via the progressive and irreversible attrition of the functional stem cell pool. They argue that prophylactic anti-inflammatory interventions may effectively delay or prevent the evolution of age-associated pathologies, but that such treatments may hold limited capacity to rejuvenate an already aged stem cell system.
In other words, it is important to reduce inflammation even during our younger years, not just during our aged period, in order to reduce stem cell aging processes. This means eating a plant-forward diet, full of lots of fruits and vegetables, as well as using sunscreen during long sun exposures, as well as using skin products that are not inflammatory – rather using skin care products that reduce inflammation and those that help to maintain or build the skin’s barrier function.
Failed company brings suboptimal skincare product to market by a manufacturer in Korea, known for fraudulent and corrupt stem cell science, even at it’s premier university, Seoul National University.
Benev is a company that couldn’t survive in the market, and had numerous problems as exemplified by this FDA review where they found poor quality control and the use of expired materials being used in production:
For example, Benev was using expired ingredients to manufacture drugs that went to market, and falsified documents to hide their egregious behavior (below is from a FDA Warning Letter to Benev):
“QCD” refers to Benev’s quality control department.
As a consequence of this violation, and may other violations, FDA concluded that Benev’s drug products were adulterated:
Resulting from continued poor performance, Benev sold themselves to a Korean company, ExoCoBio, that uses Benev to sell exosomes in the USA. A culture of corruption and fraud was highlighted by the veterinarian, Hwang Woo-suk, and his many conspirators who faked a landmark stem cell publication. That culture was exported to the USA by Benev. Previously, Benev worked with another local company called Invitrx, a company with a rich history of FDA violations, a long history, and led by a man, Habib Torfi, known for delivering stem cells to patients in a grocery bag.
There are numerous problems with what Benev (ExoCoBio) is doing to exosomes.
First, exosomes are only a fraction of what stem cells release, and without the non-exosomal fraction being combined with the exosomes, suboptimal results are achieved. In other words, when the exosomes aren’t isolated but are combined with the soluble fraction as is natural when the stem cells release their molecules, the results are superior to using only the isolated exosomes.
Second, they lyophilize their exosomes – this is a freeze-drying process that damages the molecules inside the exosome, and molecules attached to the outside of the exosome. Basically this harsh process removes all the water from the product, leaving a small amount of dry powder. The powder is full of damaged proteins and other molecules. Lyophilization leads to aggregation of proteins and their denaturization. “Unfortunately, the lyophilization process generates both freezing and drying stresses, which can denature proteins to various degrees” (Wang, 2000). Protein denaturation refers to the loss of biological activity through changes of the specific spatial conformation of protein in certain physical or chemical factors, resulting in the change of physical and chemical properties.
Lyophilization is used for the convenience of the company – it’s easier to store and ship a small pellet of lyophilized powder than it is to store and ship fresh, undamaged exosomes contained in their original solution.
From the Benev website we see they’re using lyophilized exosomes, and only the exosomes without the benefit of the soluble fraction (the overlapping text on their website is another example of the lack of attention to detail in this failed company):
To compare, NeoGenesis uses fresh (not damaged from freeze-drying) S2RM that contains both the 1. exosomal fraction, and 2. soluble fraction. Also, NeoGenesis uses both fractions from 3 cell types derived from the skin (mesenchymal stem cells and two types of fibroblasts). In contrast, Benev uses only a portion of the molecules released from one cell type, yielding a much depleted set of molecule types compared to NeoGenesis, many of which are damaged by Benev using lyophilization.
Another nearby company, Invitrx, in Lake Forest, is selling non-sterile exosomes for injection – allogenic injection. Talk about dangerous. Invitrx has a long history of unsafe practices. For example, illegally selling stem cells for injection, delivered in a paper grocery bag and selling non-sterile exosomes to physicians as exemplified in this FDA 486 Warning Letter, in which the agency details numerous non-sterile practices used to produce their exosomes.
You can read about the problems with lyophilization with many references to the published literature in my blog:
Please stop using D- and L- because it shows your profound ignorance. And, yes, both R- and S-Mandelic Acid work in the body.And, please don’t use mandelic acid with only one enantiomer as some companies want you to – it’s toxic!And please don’t drink your sunscreen – it’s stupid!
Organic compounds, molecules created around a chain of carbon atom, commonly known as carbon backbone, play an essential role in the chemistry of life. The carbon atom is unique among elements in its tendency to form extensive networks of covalent bonds not only with other elements but also with itself. Because of its position midway in the second horizontal row of the periodic table, carbon is neither an electropositive nor an electronegative element; it therefore is more likely to share electrons than to gain or lose them. In other words, it’s stable and doesn’t require the gain or loss of electrons, yet permissive because it has 4 electrons to share. Of all the elements in the second row, carbon has the maximum number of outer shell electrons (four) capable of forming covalent bonds. Other elements, such as phosphorus [P] and cobalt [Co], are able to form five and six covalent bonds, respectively, with other elements, but they lack carbon’s ability to bond indefinitely with itself. As such, carbon can form an extensive number of molecules types, and indeed, very complex molecules. These molecules are important in the energy they carry, mainly in a form of potential energy between atomic molecules. Since such potential force can be widely affected due to changes in atomic placement, it is important to understand the concept of an isomer, a molecule sharing same atomic constituents as another but differing in structural arrangement.
Stereoisomers are isomers that differ in spatial arrangement of atoms, rather than order of atomic connectivity. One type of isomer is the mirror-image stereoisomers, a non-superimposable set of two molecules that are mirror image of one another. The existence of these molecules are characterized by a concept known as chirality.
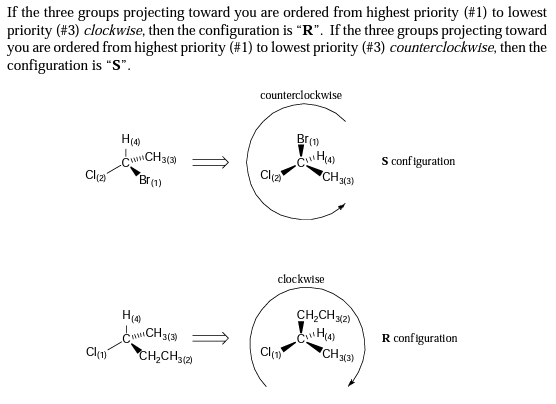
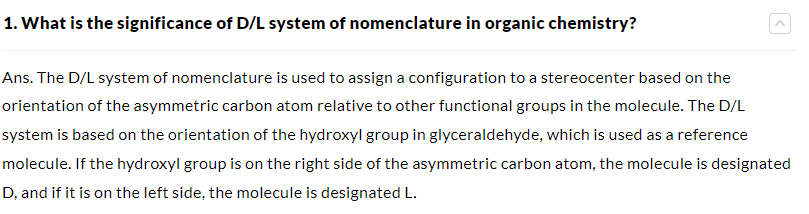
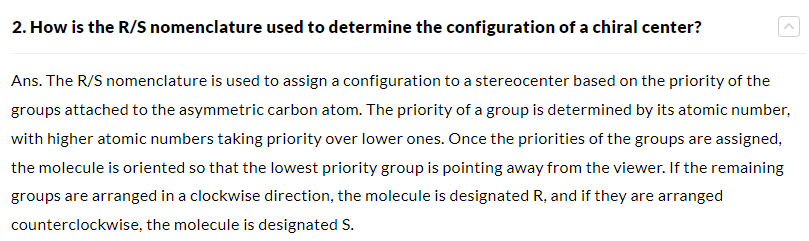
D and L configuration is an old classification that is rarely used by scientists, but is commonly used by dilletantes in the popular press and cosmetic companies who are clueless about chemistry, especially stereochemistry. D- and L- as incorrectly used by dilletantes is said to have been used to point out optical rotation in the early days that preceded a knowledge of stereochemistry. Unbeknownst to the dilletantes is that optical rotation is indicated by lowercase “d” and “l”, not uppercase. The modern way of describing chirality of molecules is the R-S system. If you want to understand how chirality is determined using the R,S system, here’s a simple guide, and a summary diagram is given below.
How did D and L originate, and why the confusion? D and L were originally used by Prof. Dr. Emil Fischer, Ph.D., in about 1891, when he was busy determining the configurations of all the sugars (glucose) by building them from d-glyceraldehyde, which has one chiral center. Chiral centers were already known to exist, although scientists were not able to determine their absolute configuration until about 1951. The idea of the chiral center was developed by a Dutch chemist, Prof. Dr. Jacobus Henricus van ‘t Hoff, Ph.D., in 1874, the first scientist to be awarded the Nobel prize in chemistry.
Prof. Dr. Emil Fischer, Ph.D., working in Germany, decided that d-glyceraldehyde was what we would now call “R”. Since his method of building sugars from D-glyceraldehyde preserved the original chiral center, he was able to determine that all the sugars he built also had D configuration in their last chiral center; that’s why we talk of “D-sugars.” In other words, building from a D-sugar led to the building of other D-sugars. Big D and Little D simply referred to sugars built from d-glyceraldehyde.
Back in the day when I lectured students about biochemistry, I would introduce D and L as a historical fact that they will have to deal with because of misinformation by non-chemists in the medical literature. Let’s review:
We now use a different system that is absolute in determining the chirality of molecules, and it uses R and S. Here’s a summary:
While the chiral (R)-mandelic acid (R-MA) is important for the drug industry because it’s a useful chiral building block for the synthesis of aromatic drugs, it is of crucial importance in the chemical and pharmaceutical industry. In humans, S-mandelic acid undergoes rapid chiral inversion to R-mandelic acid. So a racemic mixture of the R- and S- enantiomers is of little importance when using mandelic acid for topical skin applications, even if the R- and S- were shown to have different effects – and they haven’t been found to have different effects. Chiral chemicals often have functionality in both enantiomers, often with the function of each enantiomer acting at different pathways. The function of R- versus S- for many chemicals, including drugs, has not been determined.
Possible Toxicity of Using Mandelic Acid With Only One Steroisomer (enantiomer)
Here’s why you don’t want to use pure R-mandelic acid. (R)–MA is mainly synthesized chemically. The cyanide-based method involved two-step reactions including cyanation of benzaldehyde using either NaCN or transition metal catalysts, such as titanium or vanadium complexes of chiral ligands, followed by the hydrolysis of mandelonitrile using HCl to give enantiopure (R)–MA (Blacker and Houson 2002; Corson et al. 2003). This method requires the use of highly toxic cyanide and expensive transition metal catalyst together with chiral ligands but gives unsatisfied ee (meaning it doesn’t yield enantiomer excess, i.e. it doesn’t yield just the R- enantiomer), low overall yields, and generates a lot of by-products and large amount of waste. The dichloroacetophenone-based method involved the chlorination of acetophenone with chlorine, followed by alkaline hydrolysis by NaOH at 65 °C and the acidolysis with HCl. This method requires the use of toxic and dangerous Cl2, high temperature, and also suffers from side products problems (mono, tri-choloroacetophenone) (Aston et al. 2003).
Bottom line, and practically speaking, chemical methods are mainly used to produce racemic Mandelic Acid (not chiral Mandelic Acid) because it works, it’s clean (not toxic), it’s inexpensive, and it’s sustainable. It makes sense.
Having committed malpractice and losing his medical license, John Sanderson started a company called AnteAge, selling potentially dangerous products to unsuspecting victims. Negligence, repeated negligence, and sexual misconduct with his patients was his contribution to medicine. Now he wants to sell you products for your skin.He also has someone write a blog for him that not only demonstrates his total incompetence yet again, but he projects on others what he does daily – namely lie and commit unethical acts.
Mr. Sanderson is a physician who attained a bachelor’s degree in medicine from Canada. This program is 5 years in college total, and the curriculum apparently doesn’t teach ethics or compassion for others.
John Sanderson, M.B.B.S. (bachelor’s degree in medicine) who lost his medical license for negligence and repeated negligence, and sexual misconduct with a female patient.
If you want to read about Mr. Sanderson’s exploits as a practicing physician, look him up here.
I’ve selected a few excerpts shown below:
Sanderson previously was a family practice physician with an undergraduate medical degree – a bachelor’s degree in medicine. Once Sanderson finished his Canadian undergraduate degree in medicine, and once he passed the medical board test in the US, regulations permitted him to use the designation “M.D.” Sanderson frequently finds himself in disputes with other companies, one of which apparently exposed that Sanderson committed domestic violence.
Sanderson was not trained as a dermatologist and was not board certified. He obviously has little to no understanding of the skin’s powerful immune system, and no idea of how bone marrow mesenchymal stem cells work in the body. Upon losing his medical license, he started a company to do further harm to people by having them use products that induce inflammation and potentially cancer. The other physicians who is part of AnteAge and the co-blogger with Mr. Sanderson, is George Taylor, a retired anesthesiologist. Like Sanderson, Taylor has no science background and no published scientific papers. So ignorant is this guy that he has a video saying that red blood cells have no signaling capacity. That they don’t have or react to cytokines. Sorry, George. They do. I’d hate to have this sleepy guy putting me to sleep on the operating table.
Trying to understand why a company would bring a proinflammatory, possibly pro-oncogenic product to the market, I looked closer at the company. Because John Sanderson is not a scientist, and has never listed that he has any scientific publication, only misleading blogs, I wondered how did he come to choose his technology. I discovered that Sanderson had enlisted fellow Canadian, Jonathan Lakey, Ph.D. as his scientific advisor. To no surprise, the man who had lost his medical license because of incompetence had hired a scientist, Jonathan Lakey, who had been fired from his university because of fraud.
A non-profit government organization in Canada fired Jonathan Lakey for the same reason:
Then Jonathan Lakey was charged with fraud and racketeering at one of the companies in which he was an officer:
Jonathan Lakey’s involvement with a number of other companies that are pump and dump schemes has made the news a number of times. Clearly, using a product on your skin from this dynamic fraudster-incompetence duo is a bad choice – they do not have anyone’s well being in mind.
There are other skin care companies led by physicians. I suggest if you’re interested in their products, go to the state medical board website in which they practice, and look at the current status of their medical license. For example, you can search physicians in California here, and in Colorado here. You may be surprised what you find. Simply type in their name, and you’re likely to find disiplinery actions and loss of license.
Allergic diseases affect millions of people worldwide, and are on the rise. An increase in the prevalence of these diseases has been associated with alterations in the gut microbiome, i.e., the microorganisms within the gastrointestinal tract. Maturation of the infant immune system and gut microbiota occur in parallel; thus, the normal development of the microbiome likely determines tolerant immune programming in the infant. Antigens are substances that can produce an immune response, and tolerant immune programming is a mechanism of immune tolerance where the self-antigen is protected from the immune system’s destructive response. Thus the immune system is programmed to be destructive against non-self-antigens (bacteria and viruses contain non-delf antigens, for example), but not self antigens.
A new study reported that a trend in maturation alteration is characterized by depletions in the bacterial species A. hadrus, F. saccharivorans, E. hallii, and B. wexlerae in participants who later developed allergic diseases, as well as enrichments in E. lenta, C. innocuum, E. faecalis, E. coli, and T. nexilis in these participants. The depleted bacterial populations are known short-chain fatty acid (SCFA) producers, notably the butyrate producers A. hadrus, E. hallii, and F. saccharivorans and the acetate producer B. wexlerae; SCFAs are metabolites that mediate well-defined host benefits within the gut. The authors also reported a depletion of butyrate in allergy-prone participants and significant associations between A. hadrus and F. saccharivorans respective relative abundance and butyrate concentration. This strengthens the postulation that the production of butyrate and its effect on immune cells is a mode by which optimal immune modulation occurs during early life. In contrast, species enriched in allergy-prone participants have been linked to pathogenic activity and poor health outcomes, with many of these microbiome features associating with metabolites enriched within these same participants.
Most diseases are consequence of our exposome, and not hereditary genetic factors. Our exposome greatly affects our microbiome. Established primarily during infancy, the developing microbiota’s initial expansion and fluctuation are particularly sensitive to external influences before reaching a more stable community. Sensitivity of the microbiome is most pronounced during infancy, and abnormal exposures, such as that in a hospital setting, especially during a C-section, that can drastically alter the microbiome. The number of C-Sections in 2015 doubled in comparison to those registered in 2000, and jurisdictions such as California have instituted programs to stop the medical practice of performing unneeded C-sections. Indeed, many risk factors for allergic diseases, including mode of delivery, diet, urban living, and antibiotic exposure (such as the overprescribed broad spectrum antibiotic Amoxicillin), also influence early microbiota membership and structure. Note: the broad spectrum antibiotics are particularly harmful because the drug kills so many beneficial types of bacteria. While this maturation process usually coincides with the development of healthy immune tolerance, allergic sensitization can emerge in many children because of their exposome during the same period as the microbiota is being established.
Overall, the authors compared 1115 children with asthma, allergic rhinitis, food allergy, or Eczema (atopic dermatitis) to a rigorously defined, non-allergic comparator group. They described detailed underpinnings driving this decrease in gut microbiome maturation, encompassed within the alteration of a core group of bacterial species, functional pathways (i.e., potential intestinal mucous integrity breakdown, elevated oxidative stress levels, and subsequently oxidized monosaccharides, and diminished secondary fermentation), and metabolic imbalance i.e., elevated trace amines that can be involved in inflammation and neural function, and associated with reduced microbiota-maturation age and elevated risk of allergy.
Bottom line, the infant exposome is critical for the development of a normal microbiome and a life without allergy and skin conditions without Eczema.
Professor Doctor Andreas Beyer, Ph.D., at the University of Cologne, Institute for Genetics in Germany, along with his research team has discovered that as we age, a critical process in our cells, called gene transcription, speeds up. This process involves making a copy of a specific DNA strand into the form of RNA. When the process occurs too fast, more errors are made. The RNA is then used for a number of things, including making the backbone of proteins. Posttranslational modifications then finish the making of proteins.If the protein’s backbone is error ridden, the protein loses function. Likewise, posttranslational modification (PTM) depends on other proteins, and if they are error ridden, then error ridden PTM will also lead to dysfunctional proteins.
What does this mean for our health? Dr. Beyer says, for example, “Our study is saying that, for instance, having a healthy diet or, this caloric restriction intervention, would improve the quality of the transcription of the RNA production in the cell. And this would then have beneficial effects for the cells in the long run.” The evidence for his statement; mice and worms following a low-calorie diet were assessed to gauge the impact on cell transcription during the aging process. In both scenarios, transcription’s pace was observed to be more measured, resulting in fewer errors.
To validate their experiment’s applicability to humans, they conducted assessments using blood samples from both young and elderly humans. Prof. Dr. Argyris Papantonis, Ph.D., at the University of Gottingen in Germany, one of the principal investigators, remarked, “And when we compared the young cells to the very old cells, in vitro, we got exactly the same results.”
Skin aging is characterized by the accumulation of macromolecular and molecular damage within cells, impaired ability of stem and progenitor cells to promote tissue regeneration, and restore the loss of normal physiology. Chronological aging and photo-aging are two processes of skin aging that although related, have different clinical manifestations and pathogenesis. Chronological aging appears as we age and is affected by factors such as ethnicity, individual epigenetics and exposome, and skin site. It is mainly characterized by dry skin, dullness, lack of elasticity, sagging, discoloration, and fine wrinkles. Histological features include epidermal atrophy, reduction in the number of dermal fibroblasts and collagen fibers, slackening, thinness, and functional disorganization of the cells and matrix. The primary causes are: first, the stem cell dysfunction of keratinocytes, decreased regenerative ability of stem cells in the basal layer of the epidermis leading to a decline in skin renewal and repair ability, ultimately causing aging, and second, due to the accumulation of damage and aging skin dysfunction, fibroblasts lose the ability to reshape the extracellular matrix or have a reduced ability to synthesize and secrete collagen or viscous proteins. Third, aging fibroblasts alter intracellular homeostasis through certain paracrine mechanisms Now we know an important basis for these aging associated deficits is an increase in the speed of making transcripts (RNA made from DNA), and the resulting dysfunction of proteins.
As I have written, proteins being affected by our exposome is the largest factor in diseases, including cancer. A big portion of your exposome is diet. So eat well and ignore David Sinclair, your processing of transcripts in the skin will be renormalized..
Eat your vegetables, because only they can provide all the carotenoids needed by the body for many functions, including anti-cancer effects in the skin.
Carotenoids are yellow, orange, and red organic pigments produced by plants, bacteria, and algae. These pigments are important to human health, including the health of the skin, and must be acquired by diet. Carotenoids can also be fed to the skin topically. The outer layer of the skin is rich in carotenoids, and evidence finds that the sebum and perspiration naturally feed carotenoids to the epidermis. So well formulated topical products can feed the skin carotenoids too.
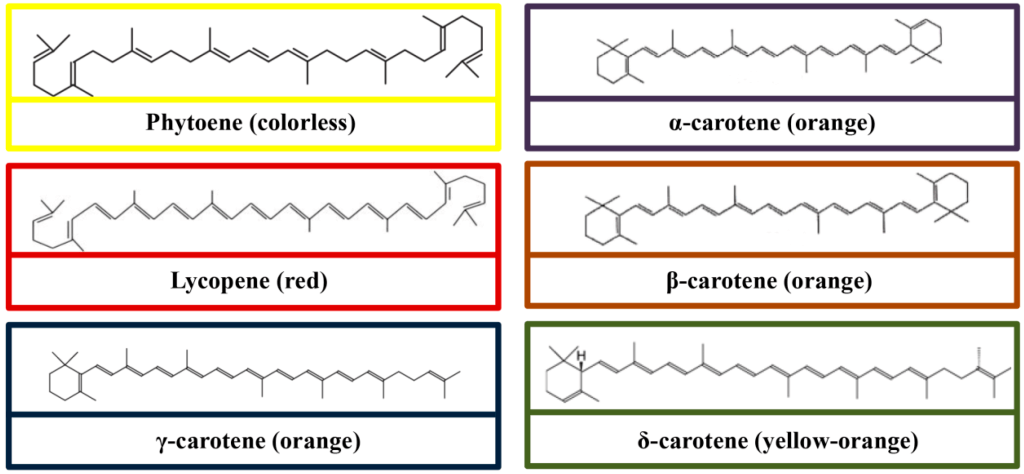
There are over 1,100 known carotenoids, which can be further categorized into two classes, xanthophylls (which contain oxygen) and carotenes (which are purely hydrocarbons and contain no oxygen). All are produced from 8 isoprene molecules and contain a backbone of 40 carbon atoms. The conjugated carbon chains of carotenoids quench singlet oxygen and other radical species. Carotenoids have antioxidant and anti-inflammatory effects in our tissues. The antioxidant and anti-inflammatory effects of carotenoids have been found to aid in the prevention of a wide range of oxidative disorders, including arteriosclerosis, obesity, and various types of cancers. In general, carotenoids absorb light wavelengths ranging from 400 to 550 nanometers (violet to green light). This causes the compounds to be deeply colored yellow, orange, or red because the violet to green colored light has been absorbed by the pigment, leaving the longer, yellow to red wavelengths of light to be seen by our eyes. In autumn, when there are fewer daylight hours and temperatures are cooler, photosynthesis slows down and there is less chlorophyll production in plants. The reduction of chlorophyll reveals yellow and orange carotenoid pigments that are usually hidden by the abundance of chlorophyll present in leaves during the growing season. Carotenoids are the dominant pigment in autumn leaf coloration of about 15-30% of tree species. Certain carotenoids that contain unsubstituted beta-ionone rings (including β-carotene, α-carotene, β-cryptoxanthin, and γ-carotene) have vitamin A activity, meaning these carotenoids can be converted to retinol in our skin.
From Tan et al (2019), molecular structures of carotenes (Phytoene, lycopene, γ-carotene, α-carotene, β-carotene, and δ-carotene).
And, molecular structures of some common xanthophylls (β-cryptoxanthin, zeaxanthin, lutein, astaxanthin, and fucoxanthin).
Human skin, is relatively enriched in lycopene and β-carotene types of carotenoids, compared with lutein and zeaxanthin. Dietary lutein and zeaxanthin are selectively taken up into the macula (central area of our retina where high contrast imaging occurs) of the eye, where they absorb up to 90% of blue light and help maintain optimal visual function. Unlike the other carotenoids, they are not precursors to retinol. Carotenoids are important components of the dark brown pigment melanin, which is found in hair, skin, and eyes. Melanin absorbs high-energy light and protects the skin from intracellular damage. β-carotene is an endogenous photoprotector, and its efficacy to prevent UV-induced erythema formation has been found in a number of studies. In the human skin, the highest concentration of carotenoids is found within adipocytes in the fat-rich subcutaneous tissue and in the stratum corneum (SC) within the lipid lamellae. The carotenoid concentration is not homogeneously distributed in the SC and has two maxima, occurring near the surface and near the bottom of the SC, which is explained by the two independent delivery pathways: from the inside due to blood circulation and keratinization, and from the outside with sweat and/or sebum secretion. Topical retinoid treatments inhibit the UV-induced, MMP-mediated breakdown of collagen and protect against UV-induced decreases in procollagen expression. Preclinical data indicate that carotenoids exhibit direct antimelanoma effect, and inhibit cell proliferation, cell migration and invasion in various melanoma cell lines grown in the lab. In a clinical study, topical carotenoids significantly enhanced skin hydration and elasticity, and reduced erythema, melanin and sebum contents over a 12 week treatment period. Several studies have observed positive effects of high-carotenoid diets on the texture, clarity, color, strength, and elasticity of skin. Beta-carotene supplementation altered skin color to increase facial attractiveness and perceived health in humans.
Let’s go a little deeper into the science when we consider our exposure to sunlight. UV radiation from the sun causes the production of free radicals in our skin. Free radicals can be particles, atoms, or molecules that have one or more unpaired electrons on the outer valence shell. This condition changes the chemistry of the molecules in our skin making them chemically very reactive. The free radical molecules try to regain their missing electron by obtaining it from the surrounding molecules. If the electron is obtained, the “stolen” electron leaves the donor molecule in a damaged state. Most free radicals contain oxygen, so they are called reactive oxygen species (ROS). The most common ROS in the biological tissues are superoxide anion radicals (O2•−), hydroxyl radicals (•OH), hydrogen peroxide (H2O2), and singlet oxygen (1O2). Also occurring are reactive nitrogen species (RNS) and lipid oxygen species (LOS) can be developed, such as lipoperoxynitrite radicals (LOO•), causing lipid peroxidation reaction cascades, inflammatory responses, and DNA and protein damage. Oxidized lipids, similar to old, rancid cooking oils that you’ve been warned not to use, can be toxic and act as lipid radicals or oxidants. The interaction of the ROS hydrogen peroxide with iron (Fenton reaction) causes chronic inflammation, sometimes leading to Ferroptosis, a form of programmed cell death. The interaction of ROS and RNS with biological molecules and cells may cause irreversible damage to their structure, which may lead to cellular dysfunction. Most of the oxygen we breath and that is consumed by cellular mitochondria in the multistep processes of oxidative phosphorylation is converted into water, while a small fraction can diffuse out of the respiratory chain as ROS and RNS. ROS and RNS are able to permeate the skin, including the stratum corneum (SC). Plasma medical procedures that damage the skin depend on this mechanism. Therefore, whether the damage is intentional, such as a medical procedure, or unintentional, such as too much exposure to the sun, carotenoids are a critical part of better preventing and remediating such damage through their antioxidant effects.
The human body, including the skin, contains a balanced set of antioxidants that can be divided into two main classes—endogenous and exogenous antioxidants. The major enzymatic endogenous antioxidants include glutathione peroxidase, catalase, and superoxide dismutase. Non-enzymatic endogenous antioxidants include glutathione, lipoic acid, uric acid, coenzyme Q10, vitamin D, intracellular reducing agents nicotinamide adenine dinucleotide (NAD), and nicotinamide adenine dinucleotide phosphate (NADP). Exogenous antioxidants enter the human organism primarily by nutrition (dietary antioxidants), such as carotenoids; vitamins A1, A2, C, and E; polyphenols (including flavonoids); zinc; and selenium Because different types of antioxidants act in synergy, significantly increasing the number of neutralized free radicals and thus improving the efficiency of antioxidant protection, ingesting and topically applying a wide variety of antioxidants, including carotenoids, is important for skin health.
The safety and benefits of soy ingredients, that preferentially activate beta estrogen receptors (ER-beta), have been known by scientists for decades. It’s time for the rest of the world to catch-up to what scientists understand.
Formulating skin care products containing various soy derivatives has led a number of people to ask me why I would use these products when there are concerns about their health risks. Unfortunately, a hysterical mass media has promulgated these ignorant ideas and social media spreads these false concerns faster and more broadly than a raging wildfire. This is something Dr. Elaine Showalter, Ph.D. taught us about back in the 1990s in her book, Hystories: Hysterical Epidemics and Modern Culture. Sadly, the phenomenon is much worse thirty years hence, benefitting the billionaire media moguls who spread alarming falsehoods with their biased algorithms, but confusing most of the rest. So let’s look at soy benefits in general first, and then I’ll describe their benefits in the skin. Once you read this, you’ll understand why I formulate with soy-based ingredients.
Let’s start with a study about the benefits of soy to general health, from Chen et al (2023) at Harvard Public Health, in a PubMed listed journal, “A higher intake of total phytoestrogens, including isoflavones, lignans, and coumarins, and foods rich in these compounds was associated with lower risk of total and certain cause-specific mortality in generally healthy US adults. These data suggest that these phytochemicals and their dietary sources may be integrated into an overall healthy diet to achieve a longer life span.” This was a large study, following nearly 76,000 women.
Soy contains compounds called isoflavones, which can act as antioxidants in the human body. Antioxidant activity may be responsible for the apparent correlation between soy consumption and lower lipid peroxidation, which can reduce the risk of arterial plaques. Higher antioxidant consumption is also associated with decreased cancer risk.
The three major isoflavones in soy—genistin, daidzin, and glycitin—all have weak estrogenic effects, acting primarily at ER-beta. Known as phytoestrogens, these compounds produce pro- or anti-estrogenic effects by binding to estrogen receptors in the body. Whereas human estrogens bind to both estrogen receptor alpha (ERα) and estrogen receptor beta (ERβ), phytoestrogens prefer ERβ, which accounts for the variations in how they affect different tissues. For this reason, phytoestrogens are referred to as selective estrogen receptor modulators, or SERMs. Selective estrogen receptor modulators affect some cells because the cells have specific estrogen receptors, while other cells are not affected because of different receptor types.
Soy derived isoflavones affect those estrogen receptors that are involved in positive effects – the ERβ subtype that is not involved in cancer. Soy blocks estrogenic effects associated with cancer because the isoflavones block ERα without activating it. Soy is inhibitory to the ill-effects of ERα.
Soy actually controls the growth of cancer cells.
Many studies have reported the anti-cancer effects of soy, for example:
The intake of soybean products in those with BRCA mutation decreased breast cancer risk 47% more than the expected risk.
The point here is that soy is safe, and beneficial in many ways including in better building bone:
Scientists in Germany showed how phytoestrogens (soy) preferentially activate ERβ:
ERβ is not located in liver or uterus, where the negative effects of estrogen have been found. Liver contains only ERα, as does the uterus. The skin contains mostly ERβ
Physiological levels of ingested phytoestrogens are safe for the uterus:
Women consuming the highest levels of soy greatly decreased their chances of cancer:
Soy consumption lessens the ill-effects of menopause:
Postmenopausal women benefit greatly from soy consumption, including better bones and muscle mass, and improved weight.
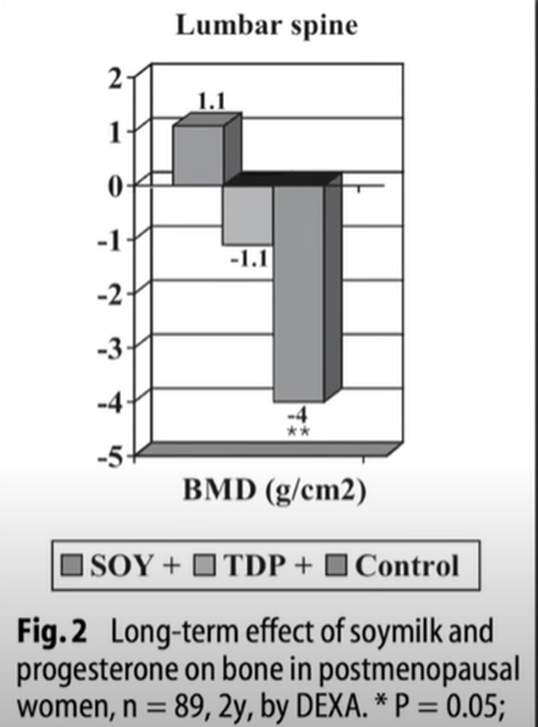
Here’s a two year study of soy milk versus progesterone or doing nothing (control) for preventing bone loss:
The results find that soy is better than progesterone or doing nothing
The benefits of soy are wide-ranging and documented throughout the world:
Soy does not feminize men – how many times have I heard this nonsense?
Soy is beneficial to children, and may decrease their incidence of cancer:
Soy benefits breast cancer survivors:
Conclusions: In this large, ethnically diverse cohort of women with breast cancer living in North America, a higher dietary intake of isoflavone was associated with reduced all-cause mortality.
Soy reduces the risk of prostate cancer in men:
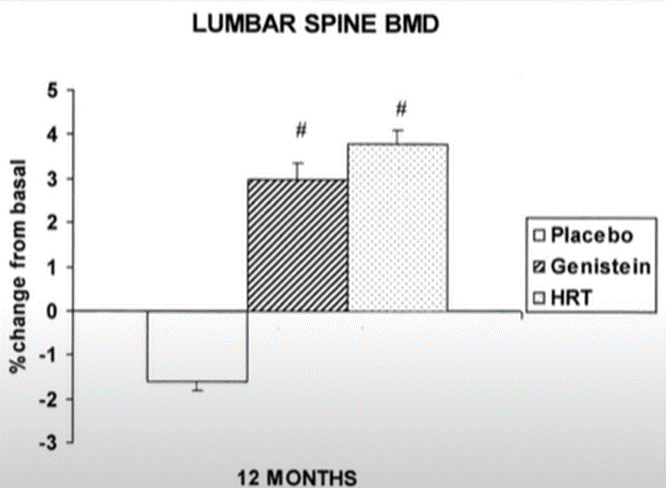
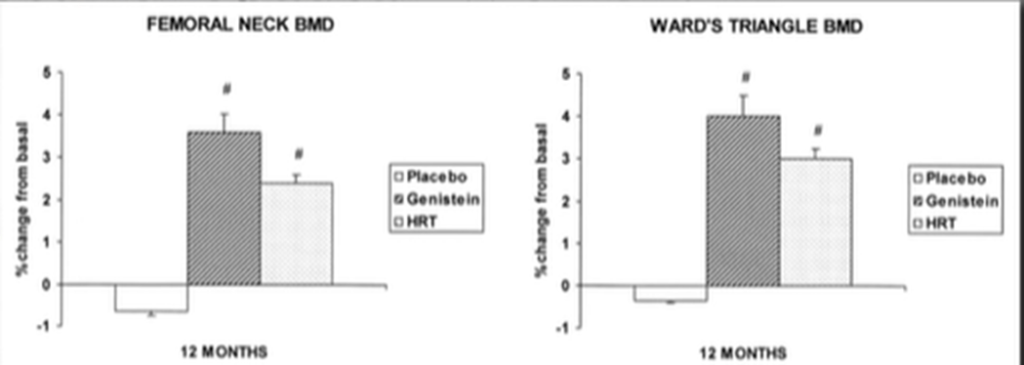
Another study of bone loss:
Results: Phytoestrogen increases bone mass equal to or better than HRT:
And this means soy lessens the chance of bone fracture in menopausal women:
Soy also benefits the skin:
Dietary soy protein supplementation with isoflavones may improve skin photoaging, including wrinkles and dyspigmentation, and increase skin hydration in postmenopausal women
The mechanisms of action through which isoflavones in soy benefit the skin are many:
Summary
Organic soy is a great addition to the diet and beenfits the body in many ways, especially as we age and estrogen levels in the body, including the skin, decline. Evidence even indicates it has anti-cancer properties.
In the land of where some people will do nearly anything for money, a company is selling “human platelet extract” as a topical cosmetic product for daily use on normal skin. Can you say, “Gee, let’s clot our skin’s blood supply, induce inflammation, and induce cancer at the same time?”Yes, extended use of a platelet extract product is likely carcinogenic (Carr et al, 2014; Sabrkhany et al, 2021). To be clear, platelet lysate (extract) triggers an inflammatory response in stem cells in the skin and induces the secretion of factors maintaining immune cells (macrophages) in a proinflammatory state thus enhancing inflammation(Ulivi et al, 2014), and long term inflammation is dangerous.
First, platelet extract does not contain exosomes as some are claiming. The company Plated uses the term “Renewosome”” to fool people. It’s marketing hype that the hysterical mass media has been repeating. They even put a trademark after this silly name. Lol. Platelet-derived exosomes (PLT-Exos) are the main subtype of extracellular vesiclessecretedby platelets, which carry proteins, nucleotides, lipids, and other substances to acceptor cells, playing an important role in intercellular communication.” Notice the term “secreted.” Exosomes are actively secreted from living platelets, and an extraction process of platelets will not yield any exosomes. None. I introduced the concept of and actual products containing exosomes to skin care over a decade ago. Many people criticized me at the time, and never bothered to read my peer-reviewed work on the subject, including my scientific book on the subject. But over a decade later following my introduction of exosomes to skin care, the word is out and people are making false claims to have exosomes in their products. Again, exosomes must be released (secreted) and cannot be collected through cellular extraction processes.
BTW, if you want to buy some human platelet extract (lysate is the scientific term for extract), here’s the source:
You can also purchase the platelet extract without fibrinogen. The company has removed the fibrinogen to reduce clotting because fibrinogen is one of the clotting factors.
So, what are platelets? Platelets are anucleated red blood cells that circulate in blood. They are small because they’re anucleated and can therefore squeeze into small places. Platelets are called into action when a wound occurs and blood is spewing. Their job is to close the wound fast by clotting to stop blood leakage, and by inducing high rates of cellular proliferation and inducing an inflammatory response to fight infection. Thus, quoting from Scherlinger et al (2023) in a Nature review article, “platelets produce soluble factors and directly interact with immune cells, thereby promoting an inflammatory phenotype. Furthermore, platelets participate in tissue injury and promote abnormal tissue healing, leading to fibrosis.” Inflammation, fibrosis, abnormal tissue healing with an abnormal matrix, and proliferation are hallmarks of cancer. Tumors are wounds that don’t heal, and applying platelet extract on your face mimics a wound that doesn’t heal. Platelets don’t live long in humans, about 7-10 days, nor would you want them to. They’ve evolved to flux into an area rapidly, secrete all of their inflammatory, clotting, and proliferative factors, close the wound, and then die before before they cause too much damage. If the platelets didn’t die, but instead stayed around for a long time secreting their inflammatory, clotting, and proliferative factors, it would be similar to applying platelet extract to your skin on daily basis. Chronic inflammation, clotting and fibrosis with tumorigenesis would result.
If we consider platelet rich plasma (PRP), a less concentrated form of platelet extract, an inflammatory response in fibroblasts is induced that leads to the formation of ROS (reactive oxygen species) and activation of oxidative stress pathways. It does not promote regeneration. Recent studies have found, “Treatment with PRP increased reticular dermis thickness with a fibrotic aspect. In the long term, the presence of inflammation and microangiopathy caused by PRP injection could lead to trophic alteration of the skin and the precocious aging process.” In other words, platelets cause fibrosis and advanced aging of the skin. Why someone would want to use platelet extract on their skin is beyond me.
According to epidemiologists, “A growing body of laboratory research has shown the direct involvement of platelets with cancer.: Cancer follows a high platelet count. Signaling by platelet-derived growth factors (PDGFs) and their receptors (PDGFRs) is commonly observed in epithelial cancers, where it triggers stromal recruitment and may be involved in epithelial–mesenchymal transition, thereby affecting tumor growth, angiogenesis, invasion, and metastasis. In other words, the extract of platelets will be high in PDGF and when applied daily will enhance the probability of cancer.
Recent studies have found that over-active PDGF signaling is implicated in several types of human malignancies, in one way by promoting proliferation, survival and invasion of tumour cells directly, and in another way by changing the tumor stroma (matrix) in a manner that promotes tumorigenesis. If we look at a product called Regranex, which is a topical product containing 0.01% PDGF, the label includes a warning, “Malignancies distant from the site of application have occurred in REGRANEX users in a clinical study and in postmarketing use.” Thus, using a platelet extract, loaded with PDGF, on a daily basis may be asking for trouble, specifically tumorigenesis.
Let’s look at the ingredients of the platelet extract product used in a “clinical study” of the platelet extract product (from their website):
Question – If the “human platelet extract” is so good, why do they need to include all of those other actives?
Answer- because the platelet extract doesn’t work well on its own. At NeoGenesis, we don’t have to add anything to our S2RM adult stem cell-based technology containing exosomes because it really works.
Let’s look at a study published by the company selling platelet extract. The study is:
This study is for short term results in treated skin, not long term results in normal skin. The study suffers from a poor experimental design, conflicts of interest, and the results are underwhelming,
First, the study was not conducted at Mayo Clinic as some people have said in social media. Rather the study was performed for payment from the company to a plastic surgeon named Steve Dyan, and the authors included those employed by the company. So Steve Dyan put his name on the paper for money – this is common, and is called ghostwriting. This is where a physician puts their name on a paper when others have done the work. He was paid to put his name on this published paper. This is a conflict of interest, and is one of the reasons why most medical research and clinical trials cannot be believed.
Look at the study design, and find the problem with the design:
Treatment Group – Before Procedure: “A 7-day pre-procedure facial skincare regimen for subjects randomized to the HPE treatment group included Cetaphil cleanser (or equivalent) twice daily morning and evening, with application of HPE once daily, and EltaMD (Colgate-Palmolive, New York, NY) UV Daily Broad-Spectrum SPF 40 (or equivalent) in the morning, with reapplication throughout the day as needed.” Treatment Group – Post-Procedure:
“Post-procedure skincare (until the skin was fully healed at 7–10 days) in the treatment group included application of HPE three times daily (morning, mid-day, and before bedtime) followed by Vanicream (PSI, Rochester, MN) Moisturizing Ointment as needed for dryness, applied 15 min after HPE CALM. Post-healing when were they [sic] determined “healed” skincare in the HPE treatment group included Cetaphil (Galderma, Fort Worth, TX) cleanser twice daily, application of HPE three times daily, sunblock, and Vanicream.”
Control Group: “Post-procedure skincare in the control group (until the skin was fully healed) included application of silicone gel twice daily and application of Vanicream Moisturizing Ointment as needed for dryness. After complete healing, the control group used Cetaphil cleanser twice daily and application of sunblock.”
Do you see the problems?
A proper study design will make the control and experimental groups the same except for the one variable, which is the test product.
Did the study do this?
No, the treatment group received extra care in the form of 7-day pre-procedure care.
Are the results convincing?
No, look at the pictures and the data – the improvement is minimal if at all.
Why didn’t the study use an active comparator? Basically this is a study of platelet extract versus doing nothing. A good study would have compared the platelet extract to something that is known to improve post-procedure healing, something like, say, NeoGenesis Recovery. The company decided to compare their product to doing nothing, and even when compared to doing nothing, the results are poor.
I could have formulated a product using platelet extract years ago, but decided not to because it is not good for the skin (inflammation and fibrosis) and is dangerous (tumorigenesis). So, if you want clotted blood vessels in your skin, tumorigenesis, fibrosis, and inflammation, go ahead and do as some company wants you to do, apply platelet extract to your face daily. Halloween is coming in a couple of months, and if you start now, you won’t need a costume.
Mesenchymal Stem Cells and their Progenitor Cells (Fibroblasts) Derived from Skin are Superior to Bone Marrow Derived Mesenchymal Stem Cells
When addressing safety and efficacy concerns of stem cells, we must consider tissue-specific stem cells. Choosing the appropriate stem cell type to match the condition to be treated is critical not only to efficacy, but most importantly, safety of the therapeutic. Beyond the genetic and epigenetic factors that influence stem cell phenotype as embryonic stem cells differentiate into somatic stem cells, the immediate niche of the stem cell will have profound influence on the cell’s phenotype. Therefore, the appropriate use of adipose derived mesenchymal stem cells (ADSCs), and their related progenitor cells from the skin, fibroblasts, is optimal for skin care compared to bone marrow mesenchymal stem cells (BMSCs)
Let’s consider some of the problems BMSCs pose for developing skin care products. The complexity of the bone marrow (BM) niche can lead to many stem cell phenotypes, whether we consider hematopoietic stem cells (HSCs) or bone marrow mesenchymal stem cells (BMSCs). Here I will discuss the properties of BMSCs, not HSCs. Because of the complexity, many BMSC phenotypes exist, including disease causing phenotypes that are varied and hard to distinguish – a part of the problem in using BMSC for therapeutic development. This complication, unlike that for ADSCS, includes recirculated cells, particularly recirculated cancer cells. Once a tumor cell disseminates into the BM, the cancer cell often displays phenotypic characteristics of BMSCs rendering cancer cells difficult to distinguish from BMSCs. BM is a site of BMSCs that may differentiate into HSCs and recirculating blood cells that may differentiate into BMSCs [see Cardenas et al; Tondreau et al]. BMSCs are also found outside of the niche in peripheral blood and home into sites of injury and cancer tissue where they are educated into becoming a pro-cancerous phenotype. Recirculated melanoma and myelogenous leukemia cells in BM interact with BMSCs to change the phenotype of the BMSC to one that is cancer promoting by enhancing their proliferation, migration, and invasion and altering the production of proteins involved in the regulation of the cell cycle. Indeed, melanoma tumor cells start to disseminate to BM during the initial steps of tumor development. In breast cancer patients, detection of recirculated cancer cells that disseminated in BM predicts recurrence of the cancer. Cancer cells can fuse with BMSCs and change their phenotype, or release exosomes to change the phenotype of BMSCs to cancer promoting. Indeed breast tumor cells fuse spontaneously with bone marrow mesenchymal stem cells. This fusion may facilitate the exchange of cellular material from the cancer cell to the BMSC rendering the fused cell more oncogenic. Further, others have found the same result of this fusion and exchange of cellular material, which has been found to increase metastasis. For example, Li et al found that human hepatocellular carcinoma cells with a low metastatic potential exhibit a significantly increased metastatic potential following fusion with BMSCs in vitro and in xenograft studies. This means that the BMSCs and their molecules/exosomes, having been conditioned by tumor cells, were found to increase the probability of cancer in human patients. The various phenotypes of BMSCs, including the cancerous phenotypes are difficult to distinguish. In contrast, even ADSCs derived from cancer patients have been found to be safe for therapeutic development.
One of many reasons why ADSCs are preferred compared to BMSCs is that ADSCs express a low level of major histocompatibility complex (MHC) class I molecules and do not express MHC class II and costimulatory molecules. Even the exosomes of BMSCs express MHC class II proteins. These problems in BMSCs are amplified when using donor, allogeneic BMSCs that have been replicated many times, essentially aging the cells, during expansion to develop the therapeutic. This is in contradistinction to ADSCs. Critically, when comparing experimental data of BMSCs to ADSCs from the same human donor, “ADSCs have a “younger” phenotype,” according to stem cell scientists. Indeed, Burrow et al found that BMSCs have, among other negative attributes compared to ADSCs, an increased level of senescence compared to matched ADSCs. Senescent cells develop the senescence-associated secretory phenotype (SASP), a pro-inflammatory set of molecules where the local tissue effects of a SASP or specific SASP components have been found to be involved in a wide variety of age-related pathologiesin vivo such as hyperplastic diseases, including cancer. Whereas the use of BMSC transplants has a history of medical adverse events, including the induction of cancer in the recipient (Maguire, 2019), fat grafting, along with its constituent ADSCs, have a long history of safety in medical procedures dating back to 1893 when the German surgeon Gustav Neuber transplanted adipose tissue from the arm to the orbit of the eye in an autologous procedure to fill the depressed space resulting from a postinfectious scar. Fat grafting’s long history of being safe, regardless of the harvesting techniques used in patients, has been recently reviewed by physician-scientists at Baylor College of Medicine. Furthermore, physician-scientists at Stanford University School of Medicine have recently reviewed the safety and efficacy of using ADSCs to augment the outcomes of autologous fat transfers. Scientists have found that ADSCs and fat grafting for treating breast cancer-related lymphedema is safe and efficacious during a one year follow-on, where patient-reported outcomes improved significantly with time. In a randomized, comparator-controlled, single-blind, parallel-group, multicenter study in which patients with diabetic foot ulcers were recruited consecutively from four centers, ADSCs in a hydrogel was compared to hydrogel control. Complete wound closure was achieved for 73% in the treatment group and 47% in the control group at week 8. Complete wound closure was achieved for 82% in the treatment group and 53% in the control group at week 12. The Kaplan–Meier (a non-parametric statistic used for small samples or for data without a normal distribution) median times to complete closure were 28.5 and 63.0 days for the treatment group and the control group, respectively. Treatment of patients undergoing radiotherapy with adult ADSCs from lipoaspirate were followed for 31 months and patients with “otherwise untreatable patients exhibiting initial irreversible functional damage” were found to have systematic improvement or remission of symptoms in all of those evaluated. In animal models with a full thickness skin wound, administration of ADSCs, either intravenously, intramuscularly, or topically, accelerates wound healing, with more rapid reepithelialization and increased granulation tissue formation, and topically applied the ADSCs improved skin wound healing by reducing inflammation through the induction of macrophage polarization from a pro-inflammatory (M1) to a pro-repair (M2) phenotype.
All in all, companies using BMSCs to develop their skin care products demonstrates a profound ignorance of the related science. Incompetence, and a greedy, lazy approach to serving the skin care market is demonstrated by those using bone marrow stem cells to develop skin care products that potentially damage their clients.