Many endogenous and exogenous factors are known to cause enlarged pilosebaceous pores. Such factors include sex, ageing, diet, chronic ultraviolet light exposure, comedogenic xenobiotics, acne, genetic and epigenetic predisposition, and seborrhoea. Most of these causative factors of enlarged pores, being exogenous and controlled by enironmental factors, means you can do something about it. There are procedures and topical products you can use to reduce pore size.
Although the pathogenesis of enlarged facial pores is still not fully understood, three factors are thought to be key to the pathology: 1) high sebum production, 2) decreased skin elasticity around pores, and 3) increased hair follicle volume. Other factors, including chronic recurrent acne, diet, sex hormones, and skin care regimens, such as inappropriate use of cosmetics, modern Western diets, washing habits, and sun exposure, also affect pore enlargement. Many of these factors will affect the epigenetics of the skin and therefore the skin’s health and potentially pore size. Epigenetics are regulated by your environment, so there is much you can do to reduce enlarged pores.
Causes of Large Pore Size
In cross-sectioned images of conspicuous, enlarged pores, a strongly undulated epidermal–dermal junction was commonly observed around a pore’s opening. Areas with this feature correlated well to the areas with larger hollows and an uneven skin tone. (Sugata et al, 2007).
Recent clinical studies have confirmed the cause of facial pore size to be multifactorial. A positive correlation of pore size and number with sebum output level has been confirmed by several studies (Roh et al, 2006; Kim et al, 2013). Enlarged pores increase with age, up to 40 years, and then stabilize or only slightly increase (Jung et al, 2018). Another significant correlation was detected between skin elasticity and pore number in two independent studies suggesting that the structure of dermis could be involved in pore widening (Kim et al, 2013; Hameed et al, 2019). Other observations found pore counts were related to wrinkle severity; and the loss of Microfibril-associated glycoprotein-1 in the hair follicle/pore area with aging and photo-exposure, indicating a lack of matrix support in the dermis (Zheng et al, 2013; Jung et al, 2018).
Both epidermal and dermal structual impairments have been identified as a cause of large pores. Microscopic imaging of pores revealed inner structural changes affecting skin, including a lower density of collagen in the deeper dermis, a thicker stroma and coarser collagen fibers forming a tubular structure around the follicle, and an irregular basement membrane ultrastructure, all of which may result in an altered distribution of skin tensions (Sugata et al, 2008; Sugiyama-Nakagiri et al, 2008; Mizukoshi and Takahashi, 2014). These ultrastructural alterations may result from inflammation, and recent data suggest inflammaging, mediated by complement activation (immune system proteins), as one of the possible inflammatory agents in the formation of enlarged facial pores (Qiu et al, 2024). Bacteria, such as Staphlacoccus aureus, infect hair follicles and pores, and the question remains, does the inflammation with this sort of infection enlarge the pore. Defects in epidermal morphology around pores have also been discovered, such as epidermis thickening and acanthosis (thickening of the stratum spinosum layer), likely indicating abnormal and possibly excessive keratinocyte proliferation ( Mizukoshi and Takahashi, 2014).
Procedures to Reuce Pore Size
Procedures, such as Micro-focused ultrasound with visualization (MFU-V), have been found to reduce pore size. MFU-V uses focused ultrasound energy to lift and tighten the skin by delivering heat to specific tissue layers beneath the skin’s surface, stimulating collagen production and causing skin tightening according to The Journal of Clinical and Aesthetic Dermatology. The visualization aspect of the procedure allows practitioners to see the underlying tissue during treatment, ensuring precise targeting and optimal results.
Topical S2RM to Reduce Pore Size – It’s Not Just the Exosome, It’s the Secretome
But are procedures needed to reduce pore size? No, the right choice of topical skin care products can significantly reduce pore size too. The secretome from adipose mesenchymal stem cells, something used in the NeoGenesis S2RM technology, significantly reduces pore size. That inflammation inducing the ultrastructual changes causing pores to enlarge can be reduced- reduce the inflammation with ADSC secretome found in the NeoGenesis S2RM technology. Remember,It’s Not Just the Exosome, It’s the Secretomethat is optimal for reducing inflammation and regenerating tissue – including the tissue that constructs the pore. Changes of TEWL found that ADSC secretome can faciltate the recovery of the skin barrier function (Zhou et al, 2013), which can be explained by ADSC secretome normalizing the proliferation and migration of human primary keratinocytes as reported by Moon et al (2012). Both the epidermis (Ren et al, 2024) and dermis (Silveira et al, 2022) and hypodermis (An et al, 2021) are regenerated by ADSC secretome, with ADSC secretome containing collagen type IV needed to build the basment membrane, thereby regulating that “undulated epidermal–dermal junction” found to underly increased pore size.
I want to emphasie that inflammaging, inflammation that occurs as we age, is exposome induced. Those who eat well and live in an healthy envionment don’t suffer from inflammaging (Franck et al, 2025). As Franck et al write, “Inflammaging, as measured in this manner in these cohorts, thus appears to be largely a byproduct of industrialized lifestyles, with major variation across environments and populations.” In other words, if you live a healthy lifestyle, chronic inflammation, including inflammaging, is something you won’t suffer. This will reflect in your skin health, and your skin’s pore size.
Summary
Pore size in the skin depends on your envionment, your so-called exposome. Healthy skin is beautiful skin, including beautiful, healthy pores. Eat well to keep the skin healthy with sebum production levels normal and therefore reducing a risk factor for increased pore size. And the right choice of topical skin care products can help keep the skin healthy and pore size normal.
Inflammation is for fighting pathogens, and it is destructive to the skin. Inflammation is not needed to regenerate the skin or induce collagen production, and actually slows and impedes the healing process.There is a potent and safe means to inhibit the inflammatory pathways and promote regenerative healing in the skin -S2RM Technology- stem cell released molecules from skin derived adipose mesenchymal stem cells and fibroblasts.
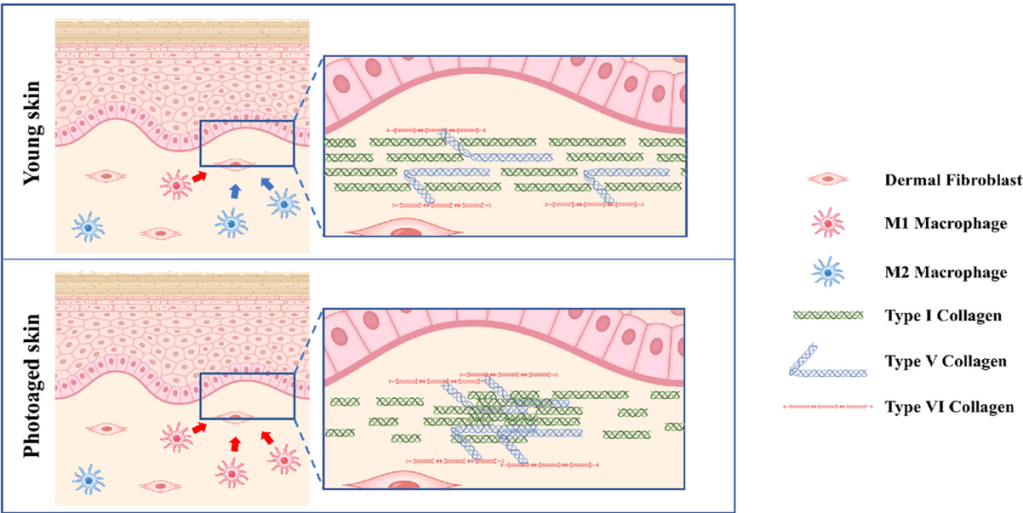
From: Liu et al 2017
I continuously hear that inflammation is needed to heal the skin and to produce collagen and rebuild the matrix. This is false, and I’ll tell you why, and tell you the differences in the two healing processes, i.e 1. non-inflammatory regenerative healing versus, 2. inflammatory reparative healing.
Once we’ve exited the sterile or nearly sterile womb, most postnatal wounds heal through reparative healing, which is a complex biological process involving cells, signaling molecules such as growth factors and other cytokines, and the extracellular matrix (ECM). Wound healing is simplified and described as occurring in four overlapping, highly coordinated stages: hemostasis, inflammatory, proliferation, and remodeling. In the womb, where there are no pathogens, inflammation is not needed to fight infection – there’s no pathogens present to infect the skin. In the fetus, the immune system in the skin is only beginning to develop and is not robust, and platelets that normally rush into wounded skin are not yet fully developed, and the blood cells are being produced in the liver and not in the bone marrow. Wound healing in the fetus is vastly different from that in the adult. Adipose mesenchymal stem cells (AMSCs) arise later in fetal development in order to control and resolve the newly formed inflammatory mechanisms in the skin that are important in the adult to fight infection using an inflammatory response.
Whether it is macrophages or T cells, including γδ T-cell subsets, or other immune cells, it is the AMSCs that serve to calm the early-onset inflammation by polarizing the immune cells from an inflammatory type to an anti-inflammatory, pro-regenerative type. This is in contrast to bone marrow mesenchymal stem cells (BMSCs), which are a major source of IL-7, thus producing inflammation, and playing a pathological role in the maintenance of inflammatory CD4 memory T-cells that are involved in autoimmunity and chronic inflammation. BMSCs and the molecules they release also have oncogenic potential, another reason why they are an inferior choice for therapeutic development.
Regenerative Non-Inflammatory Healing and Reparative-Inflammatory Healing
Fetal wounds heal in utero through regenerative healing; postnatal microenvironments with an attenuated inflammatory response, such as the oral mucosa, also heal with regenerative characteristics, including a reduced immune response and scarring. Regenerative healing occurs in a manner similar to the same four stages of reparative healing, with some key differences. The key difference is that compared with reparative healing, the inflammatory response in regenerative healing is attenuated. Many of the cells involved in both innate and adaptive immunity, such as mast cells, macrophages, and neutrophils, are not yet differentiated or are not responsive to the wound where regenerative healing occurs. Therefore, levels of inflammatory cytokines and chemokines are reduced or absent in regenerative healing.
Increased expression of anti-inflammatory cytokine IL-10 in postnatal regenerative healing helps decrease the inflammatory response. Adipose mesenchymal stem cells are a key source of the IL-10 secreted into the skin, and thus promoting regenerative healing. A number of studies suggests that IL-10 not only indirectly modulates fibrosis via its anti-inflammatory properties but may also stimulate fetal-like fibroblast behavior and thus fetal-like ECM production. If scar tissue is to be of normal structure, regenerative healing must take place. The secretion of IL-10 from AMSCs is key to inducing regenerative healing in adult skin. One mechanism to explain the ability of IL-10 to inhibit inflammation is that it inhibits NF-κB activity by inhibiting nuclear translocation of NF-κB by blocking IκBα degradation in response to TNF stimulation.
Collagen Production in Wound Healing – Inflammation Degrades Collagen, Not Produce It
Collagen production in the skin to aid in healing, is mainly derived from fibroblasts, but also by keratinocytes. Fibroblasts have evolved to regulate their synthesis of collagen and other extracellular matrix proteins in response to mechanical tension. Fibroblasts are also induced to secrete collagen by the molecules released from AMSCs. It’s not inflammation that stimulates the production of collagen. Tissue damage caused by inflammation from an infection or an autoimmune disease triggers degradation of collagen in the extracellular matrix (ECM), which further enhances inflammation. So inflammation is degrading collagen, not producing it. Also know that dermal collagen has a half-life of about 15 years, a very long-lived protein, a feature that predisposes collagen to accumulate lesions such as advanced glycosylation end products (AGE), which have damaging effects on the molecules they bind. So with much collagen in the skin lasting for decades, accumulating damage through inflammation is occurring. The secretome from AMSCs can protect these long-lived collagen proteins from inflammatory damage, while also helping to replace damaged collagen.
Non-Inflammatory Immune Cells, M2 Macrophages are Anti-inflammatory and Pro-Regenerative
Often, the delay in tissue healing results from the inflammatory phase of the wound healing. Non-healing wounds result from chronic inflammation, characterized by an overload of inflammatory immune cells, inflammatory cytokines, and proteolytic enzymes. Chronic wounds share certain common features, including excessive levels of proinflammatory cytokines, proteases, ROS, senescent cells, persistent infection, and a deficiency of stem cells and their released molecules that are often also dysfunctional. Chronic wounds are defined as wounds stalled in a constant and excessive inflammatory state. For example, much evidence has revealed that chronic wounds are closely associated with impaired phenotype transition of pro-inflammatory macrophages (M1) to anti-inflammatory phenotypes (M2) in wounds. The secretome from AMSCs biases the macrophage phenotype from an inflammatory M1 to an anti-inflammatory, pro-regeneration M2 phenotype, and greatly aids in wound healing. An example of the pro-healing effects is that M2 macrophages induced the expression of the proteins required for the assembly of collagen fibrils, and macrophages themselves secrete some forms of collagen. A shift towards M2 in the M1/M2 balance improves not only the quantity but also the quality of collagen fibrils, leading to a non-fibrotic scar. M2 macrophages induce the expression of the proteins required for the assembly of collagen fibrils,
From: Horiba et al (2023)
In wounds, the continued infiltration of pro-inflammatory immune cells and production of pro-inflammatory molecules attract additional inflammatory immune cells, exacerbating the inflammation. Thus, inflammation is preventing wound healing. If you think inflammation is needed to clear debris in a wound, including “sterile inflammation,” think again. During the resolution of inflammation, macrophages are predominantly polarized to an M2 phenotype (non-inflammatory), which can suppress proinflammatory cytokine production, clear debris, and restore tissue homeostasis. Yes, M2 macrophages are phagocytic – meaning they eat debris. Again, wounds don’t need inflammation to heal, whether it’s an infected wound, or “sterile inflammation” where debris is present without infection.
The Inflammatory NK-kB Pathways Are Pro-Inflammatory and Impede Wound Healing
Recent studies have found the genes and pathways involved in the induction of inflammation, called, NF-kB, and that these genes and pathways are also involved in aging and many disease processes. The NF-kB pathways underlying inflammation, diseases, and aging (inflammasome) are different from the genes and pathways that are activated during injury and responsible for regenerative healing.
Leung et al (2013) at Stanford did a nice study separating out the two pathways involved in adult healing, i.e. the NF-kB pathways. They found that hypochlorite (HOCl) reversibly inhibited the expression of CCL2 and SOD2, two NF-κB–dependent genes. In radiation dermatitis, topical HOCl (aka Bleach) inhibited the expression of NF-κB–dependent genes, decreased disease severity, and prevented skin ulceration. Additionally, skin of aged HOCl-treated mice acquired enhanced epidermal thickness and proliferation, comparable to skin in juvenile animals. In other words, inhibiting inflammation helped to heal the skin when injured through irradiation or aging.
Platelets, Bone Marrow Mesenchymal Stem Cells, and Their Molecules Induce Inflammation
This is why you don’t want to use a platelet extract or PRP on your skin, because platelets and their molecules induce inflammation. It’s also why you don’t want to use bone marrow mesenchymal stem cell derived molecules because they too are pro-inflammatory and can induce, through IL-7, autoimmunity and tissue destruction. Both of these cell types only appear transiently in open wounds through the blood supply and serve to induce inflammation to fight infection, and to induce high rates of fibrotic scarring to close the wound rapidly (see Maguire, 2022).
Adipose Mesenchymal Stem Cells and Their Molecules Reduce Inflammation
There’s another safe and effective means to inhibit the inflammatory pathways associated with NF-kB, and that is the secretome from AMSCs, which is contained in the S2RM Technology of NeoGenesis.González-Cubero et al (2022) in Spain found that in inflamed human cells from connective tissue, like that found in the skin, when exposed to the molecules released from AMSCS, NF-κB activation was blocked. Thus, the secretome from AMSCs blocked inflammation by blocking the NF-kB pathways. Adipose mesenchymal stem cells and their released molecules act in many other ways in addition to inhibiting NF-kB to reduce inflammation.
Chronic Inflammation
So the adipose mesenchymal stem cells reduce inflammation and this is critical for autoimmunity. Tregs control other T cells from over activating and causing damaging inflammation. It is important to keep Treg cell functioning because they tend to lose their regulatory capacity under chronic severe inflammatory conditions. If a patient’s Treg cell function is compromised or defective, their immune system can become excessively activated, leading to systemic autoimmune inflammation. So AMSCs controlling inflammation in turn controls Treg cell function and reduces T cell mediated autoimmune inflammation.
Summary – Inflammation is Unwanted in Wound Healing and Adipose Mesenchymal Stem Cells Deactivate Inflammation and Activate Regenerative Healing
In summary, inflammation does not heal the skin and does not produce collagen. Inflammation is unwanted in the skin unless their is an infection and the pathogens need to be destroyed. Unfortunately, in the process of killing the pathogens, the inflammation also damages your cells and connective tissues. To effectively and safely decrease inflammation and activate regenerative wound healing, use NeoGenesis Recovery which is loaded with the molecules released from AMSCs that reduce inflammation and activate pro-healing regenerative mechanisms.
Psoriasis is a relapsing–remitting immune-mediated skin disorder characterized by epidermal overgrowth, and massive inflammatory infiltrates as hallmarks of scaly erythematous lesions. Epigenetic changes detected in epidermal keratinocytes of resolved skin may be responsible for the DRTP (disease-residual transcriptomic profile) in the same regions, leading to a reoccurrence of the lesion. I’ll explain some ways, including new technologies for epigenetic regulation, to better treat psoriasis.
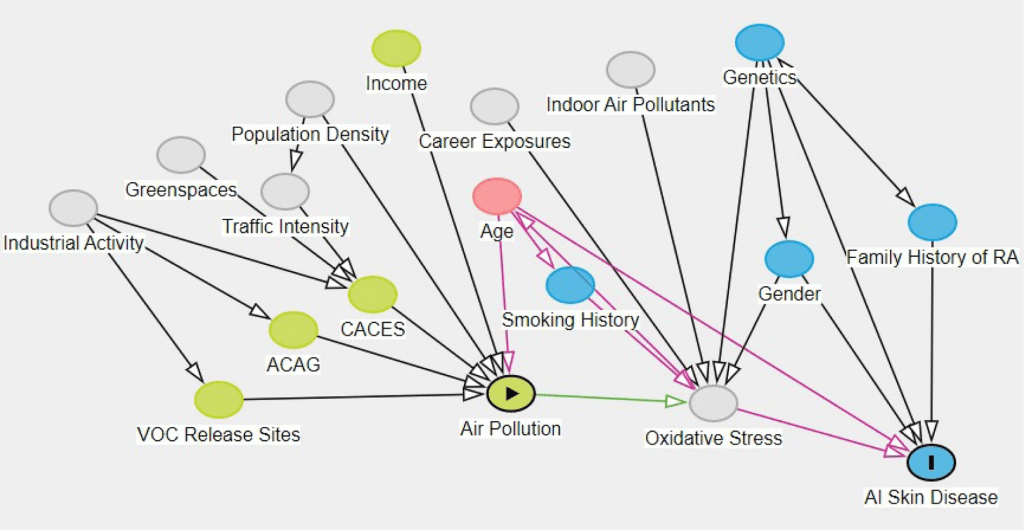
The multifactorial causes of inflammatory skin conditions, including psoriasis. From: Lowe et al (2022)
Like most diseases, psoriasis is environmentally triggered. You can think of it as mismatch between hereditary factors, including but not just genetics (Bonduriansky, 2012), and the environment. The modern environment is full of triggers for psoriasis, such as air and water pollution (Lowe et al, 2023) and poor diets (Kanda et al, 2020), and our hereditary factors have not adapted to the new environment. With over 2,000 new chemicals introduced into the USA each year, genetic based heredity will never adapt us to our ever changing environment. Evolutionary adaptation based on genetics requires too much time, usually at least thousands of years. For example, the recent introduction of eating processed food with high amounts of salt (sodium) can lead to sodium accumulation in the skin, and can be an inflammatory factor in psoriasis (Maifeld A et al, 2022), dramatically impeding skin remodeling (Pajtók et al, 2021). People haven’t yet adapted to high levels of dietary sodium, and so it is causative, at least partially, in many diseases (Lucarini et al, 2021), including psoriasis.
An example of the slow genetic hereditary adaption to the environment is lactose tolerance in some populations of humans where the environment included cattle and the milk they made available to humans. Studies of DNA from 40,000 years ago up to a few hundred years ago show that there has been a very rapid rise of the genetic variant that helps humans consume milk as adults, called lactose tolerance. The genetic variant didn’t become common until the past 1,000 to 2,000 years. With thousands of years of heredity, humans who co-evolved with cattle developed the ability to drink the milk of cattle. In East Asia, where cattle were not common, the people remained lactose intolerant (Goh et al, 2018).
However, and important to disease states such as psoriasis (Dopytalska et al, 2021), epigenetics, another hereditary factor that is not genetic, can play significant and rapid roles in adaptation to the environment (Carneiro et al, 2020). Epigenetics is not changes in the DNA itself, rather it is environmentally triggered changes in the expression of DNA. In other words, epigenetics is about what DNA is turned-on or turned-off by environmental factors. These genetic and epigenetic adaptations can turn out to be maladaptive given the rapid and ever changing environment in today’s modern world. That is, you epigenetically adapt to one thing in the environment, but another thing comes along in the environment that is a mismatch for the epigenetic adaption. That epigenetic maladaptation can pass on to your offspring and their offspring (Fitz-James and Cavalli, 2022). But there is good news. Scientists in Germany have demonstrated that maladaptive epigenetics in human skin can be reversed to some degree by using naturally sourced DNA methylation inhibitors , leading to better skin health (Falckenhayn et al, 2024). Methylation is one of the key means by which DNA can be turned-on of turned-off.
Considering psoriasis, like most bodily functions, epidermal desquamation is a highly regulated process of corneocytes shedding from the outermost layers of the stratum corneum (Haftek, 2015). Psoriasis is a condition where skin cells replicate at an abnormally fast rate. This leads to a buildup of dead, interconnected skin cells on the surface, forming the thick, silvery plaques and a lack of moisture that characterize this condition. Normal shedding of corneocytes is disrupted, leaving a thick patch of dried skin tissue.
So let’s look at how we can renormalize the physiology of psoriatic skin using three key topical products currently on the market, and one that will be released soon.
Salicylic acid (SA)
Salicylic acid (SA) is a keratolytic that promotes stratum corneum desquamation (Elmets et al, 2021). Evidence suggests that SA works by digesting skin keratin and disrupting barriers to water-binding functions that allows the skin plaques to desquamate (Rawlings et al, 1994). Like the enzymes involved in filaggrin degradation, the hydrolases (enzymes that depend on water to breakdown the structures) involved in desmosome degradation and lipid degradation are dependent upon water for their activity. However, water activity within the stratum corneum is dependent upon the NMF and lipids. When adversely influenced by many factors, such as degraded barrier function, insufficient stratum corneum moisturization and water content leads to defective desquamation.
SA works best when an occlusive and moisturizing formulation is applied on top of the salicylic acid gel, thereby creating an environment optimal for barrier repair, where moisture is retained, thus maximizing normal enzyme activity and minimizing the irritating effects of SA.
At Neogenesis, we use an OTC drug form of SA that contains 2% salicylic acid. This is a mild form of SA and can be used daily for moderate to severe forms of psoriasis. Stronger forms of salicylic acid, which have side effects, are available by prescription from your dermatologist. As for all drugs, follow the OTC label on all salicylic acid products before applying.
2. Moisturizers
Considering the NMF and lipids that are important for treating psoriasis, NeoGenesis’ Barrier Renewal Cream (BRC) features NMF and lipid ingredients critical to barrier repair and remediating psoriasis. These ingredients include, Urea, Squalane, Caprylic/Capric Triglyceride, Safflower Oleosomes, Glycerin, Sodium PCA, Ceramide NP, Ceramide AP, Ceramide EOP, Phytosphingosine, Cholesterol, and Sodium Hyaluronate Butyrate. Not only is BRC providing necessary lipids and NMF to rebuild the epidermal barrier, but butyrate is another key molecule for epidermis. Butyrate, originating from gut bacteria and skin bacteria, has been found to increase Treg and reduce inflammation in the skin (Schwarz et al, 2017), regulate mitochondrial function of keratinocytes (Trompette et al, 2022) and to increase the expression of FLG protein by inhibiting the activity of histone deacetylase, and restoring the function and permeability of the epidermal barrier (Kleuskens et al., 2022).
3. S2RM – Stem Cell Released Molecules
The molecules in S2RM inhibit the proliferation of activated T cells, modulate the release of inflammatory cytokines and chemokines by dendritic cells and macrophages, suppress proliferation and immunoglobulin production of B cells, and inhibit cytotoxic activity of natural killer (NK) cells. The positive effects of topically applied stem cell released molecules in psoriasis are dramatic and occur quickly (Seetharaman et al, 2019). Controlling all of these functions in psoriatic skin using S2RM is highly important to controlling inflammation and autoimmunity.
4. Something New – Autoimmune, DNA Methylation Modulators
Epigenetic mechanisms of gene expression regulation are a group of the key cellular and molecular pathways that lead to inherited alterations in genes’ activity without changing their DNA coding sequence. Methylation of cytosine residues in the CpG island located in the gene promoter region of DNA causes suppression of gene expression, while these unmethylated regions of DNA leads to activation of gene expression. Modulation of methylation can therefore turn on or turn off gene expression and in this way remove or modify epigenetic “memories.” In this way, if the cells of the skin have an epigenetic memory of a chronic inflammatory event, for example, epigenetic modulators can eliminate or reduce this memory.
I won’t go into details here, but many long coding RNAs are involved in the immunopathogenesis of psoriasis (Tsoi LC et al, 2015), and long non-coding RNA (lncRNA) mediates DNA methylation in both physiological and pathological conditions (Huang et al, 2022). A lncRNA named PRINS (Psoriasis susceptibility-related RNA Gene Induced by Stress) has been found to be essential in the survival of keratinocytes under stress condition and is thought to contribute to psoriasis susceptibility (Sonkoly et al, 2005). Epigenetic changes detected in epidermal keratinocytes of resolved skin may be responsible for the DRTP (disease-residual transcriptomic profile) in the same regions, leading to a reoccurrence of the lesion (Ghaffarinia et al, 2023) . If the epigenetic changes in keratinocytes can be erased, then the reoccurrence of the psoriatic lesions may be abated.
Falckenhayn et al (2024) found that natural, plant-based DNA methylation inhibitors were able to penetrate the skin. For example, they found dihydromyricetin, which (for you chem nerds) has a molecular weight of 320.25 g/mol and a logP of 1.23 (ChemSpider) was able to penetrate into living skin cells. The positive effects they found included increased epidermal thickness and a more youthful set of cellular parameters. As a result, fewer wrinkles (3.7 tears of wrinkle accumulation were removed) were found in treated skin compared to controls. Other natural ingredients, including cannabinoids have been found to modulate DNA methylation and reduce skin autoimmunity and inflammation.
Cannabinoids are of great interest to me because I personally know the power of the endogenous cannabinoid systems in the body. When I was professor at UCSD, my lab discovered the cannabinoid signaling system in the eye, and later found with colleagues at UCSB that when the endogenous cannabinoid system is fully activated, neurons, called retinal ganglion cells, are protected from neurodegeneration. It is indeed, a very powerful system throughout the body involved in immune function and epigenetics.
For example, the first evidence describing the possible effects of CBD and CBG on DNA methylation aimed at clarifying the epigenetic regulation of keratinocyte differentiation by phytocannabinoids. Their study used human kHaCaT cells, revealing that CBD increased global DNA methylation and decreased gene expression involved in keratinocyte differentiation. In other words, CBD and CBG slowed down replication of keratinocytes. Again, psoriasis is characterized by an excessive proliferation and abnormal differentiation of keratinocytes and infiltration of multiple inflammatory cells. Interestingly, CBD effects on DNA methylation and gene expression were mimicked by AEA and blocked by a selective CB1 antagonist, suggesting an indirect mechanism rather than a direct regulation by CBD (Pucci et al, 2013). Many people haven’t heard about the power of CBG, but it is a very powerful antioxidant and anti-inflammatory in the skin (Perez et al, 2022).
I’ll tell you more about it later, but we currently have a product in testing that features a number of phytochemicals, including CBD and CBG and other epigenetic modulators. It’s sure to help a number of inflammatory skin conditions, including psoriasis. Stay tuned.
References
Bonduriansky R. (2012) Rethinking heredity, again. Trends Ecol Evol. 27(6):330-6
Carneiro VC et al (2020) Rapid Epigenetic Adaptation in Animals and Its Role in Invasiveness, Integrative and Comparative Biology, Volume 60, Issue 2, Pages 267–274,
Dopytalska K, Ciechanowicz P, Wiszniewski K, Szymańska E, Walecka I. The Role of Epigenetic Factors in Psoriasis. Int J Mol Sci. 2021 Aug 27;22(17):9294.
Elmets CA et al. (2021) Joint AAD-NPF Guidelines of care for the management and treatment of psoriasis with topical therapy and alternative medicine modalities for psoriasis severity measures. J Am Acad Dermatol. 84(2):432–470.
Falckenhayn C et al (2024) Identification of dihydromyricetin as a natural DNA methylation inhibitor with rejuvenating activity in human skin. Front Aging. 4:1258184.
Fitz-James, M.H., Cavalli, G. (2022) Molecular mechanisms of transgenerational epigenetic inheritance. Nat Rev Genet23, 325–341.
Ghaffarinia A et al (2023) Psoriatic Resolved Skin Epidermal Keratinocytes Retain Disease-Residual Transcriptomic and Epigenomic Profiles. Int J Mol Sci. 24(5):4556
Goh LH et al (2018) Lactase deficiency and lactose intolerance in a multiracial Asian population in Malaysia. JGH Open ;2(6):307-310.
Haftek M. Epidermal barrier disorders and corneodesmosome defects. Cell Tissue Res. 2015 Jun;360(3):483-90.
Huang, W., Li, H., Yu, Q. et al. (2022) LncRNA-mediated DNA methylation: an emerging mechanism in cancer and beyond. J Exp Clin Cancer Res41, 100.
Kanda N, Hoashi T, Saeki H. Nutrition and Psoriasis. Int J Mol Sci. 2020 Jul 29;21(15):5405.
Lowe, M.E et al (2023) The skin is no barrier to mixtures: Air pollutant mixtures and reported psoriasis or eczema in the Personalized Environment and Genes Study (PEGS). J Expo Sci Environ Epidemiol 33, 474–481.
Lucarini M et al (2021) Sodium Intake and Related Diseases. Int J Mol Sci. 22(14):7608
Maifeld A et al (2022) Skin Sodium Accumulates in Psoriasis and Reflects Disease Severity. J Invest Dermatol. 142(1):166-178.e8.
Pajtók C, Veres-Székely A, Agócs R, Szebeni B, Dobosy P, Németh I, Veréb Z, Kemény L, Szabó AJ, Vannay Á, Tulassay T, Pap D. (2021) High salt diet impairs dermal tissue remodeling in a mouse model of IMQ induced dermatitis. PLoS One. 16(11):e0258502.
Perez E, Fernandez JR, Fitzgerald C, Rouzard K, Tamura M, Savile C. (2022) In Vitro and Clinical Evaluation of Cannabigerol (CBG) Produced via Yeast Biosynthesis: A Cannabinoid with a Broad Range of Anti-Inflammatory and Skin Health-Boosting Properties. Molecules. 27(2):491.
Pucci M et al (2013) Epigenetic control of skin differentiation genes by phytocannabinoids. Br J Pharmacol. 170(3):581-91.
Schwarz A, Bruhs A, Schwarz T (2017) The Short-Chain Fatty Acid Sodium Butyrate Functions as a Regulator of the Skin Immune System. J Invest Dermatol. 137(4):855-864.
Seetharaman R et al (2019) Mesenchymal Stem Cell Conditioned Media Ameliorate Psoriasis Vulgaris: A Case Study. Case Reports in Dermatological Medicine. Volume 2019 | Article ID 8309103.
Sonkoly E et al (2005) Identification and characterization of a novel, psoriasis susceptibility-related noncoding RNA gene, PRINS. J Biol Chem. 280(25):24159-67.
Trompette, A., Pernot, J., Perdijk, O. et al. (2022) Gut-derived short-chain fatty acids modulate skin barrier integrity by promoting keratinocyte metabolism and differentiation. Mucosal Immunol15, 908–926.
Tsoi LC et al (2015) Analysis of long non-coding RNAs highlights tissue-specific expression patterns and epigenetic profiles in normal and psoriatic skin. Genome Biol. 16(1):24.
Studies at Mayo Clinic provide evidence that the molecules we use at NeoGenesis repair spinal cord injuries in human patients. Injecting AMSCs into the spinal cord of patients with traumatic spinal cord injuries yielded positive outcomes, including changes in sensory and motor scores, imaging, cerebrospinal fluid markers, and somatosensory evoked potentials. The positive results were attributed to the molecules released by the AMSCs, the same molecules used in S2RM and previously demonstrated by my lab to protect and repair neurons.
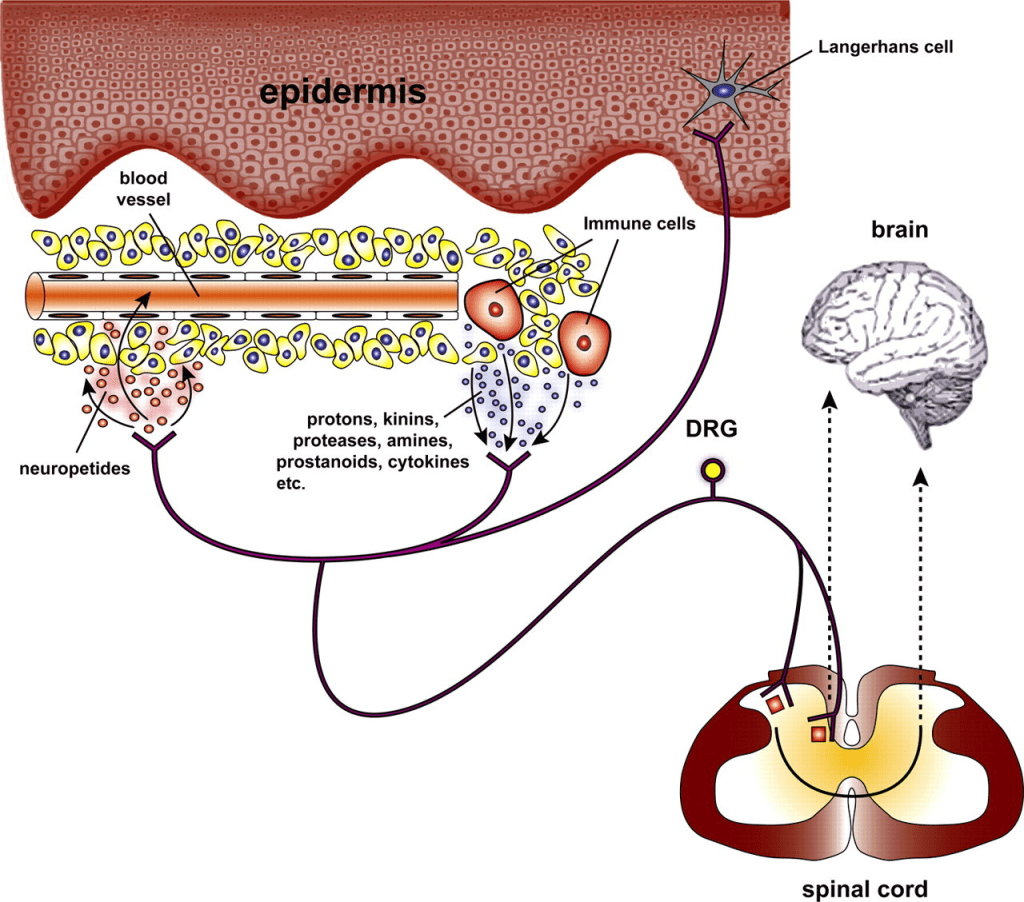
From: Roosterman et al (2006)
S2RM, based on the molecules that AMSCs and fibroblasts secrete, is a powerful and safe technology. The power of S2RM to benefit the nervous system is one of many mechanisms by which the molecules provide therapeutic actions in the skin. Why? Cutaneous neuroimmunoendocrinology is involved in several skin diseases. That’s a big word used by scientists. It means that the nervous system, the immune system, and endocrine system are all connected. The central nervous system (CNS) is directly, through efferent nerves or CNS-derived mediators, or indirectly, through the adrenal glands or immune cells, connected to skin function.
The skin is innervated by afferent (nerve fiber carrying signal from the skin to the brain) somatic nerves with fine unmyelinated (C) or myelinated (Aδ) primary afferent nerve fibers transmitting sensory stimuli (temperature changes, chemicals, inflammatory mediators, pH changes) via dorsal root ganglia and the spinal cord to specific areas of the CNS, resulting in the perception of pain, burning, burning pain, or itching. It’s a powerful system, and when function goes awry, it can drive you crazy – for example, itching and burning of the skin.
I’ll be nerdy here and explain the brain connection to the skin underlying itch (pruritis), as described by Roosterman et al (2006) in Physiological Reviews. In pruritus, skin-derived itch-selective primary afferent fibers are connected with specific units within the lamina I of the spinal cord. Here, they form a distinct pathway projecting to the posterior part of the ventromedial thalamic nucleus (nerves projecting from spinal cord to midbrain). The pathway then projects to the dorsal insular cortex that is involved in a variety of interceptive modalities such as thermoception, visceral sensations, thirst, and hunger. As revealed by functional positron emission tomography (fPET imaging technology), induction of itch by intradermal histamine injections and histamine prick induced coactivation of the anterior cingulate cortex, supplementary motor area, and inferior parietal lobe, predominantly in the left hemisphere. This considerable coactivation of motor areas explains the common observation of itch being essentially linked to a desire to scratch. In other words, the afferent “itch signals” from the skin to the brain lead to efferent “scratch signals” from the brain to the periphery (hands).
As you can see, a functional spinal cord is needed for all of this skin-brain signaling to work. And if there is damage to any of these nervous system areas, the peripheral nervous system in the skin, the spinal cord, or the brain itself, S2RM can help to repair it! That’s part of the power of S2RM.
The S2RM technology that I developed is based on the molecules released from skin derived adipose mesenchymal stem cells (hASCs) and fibroblasts (HNDF). This combination of many molecules has many benefits to the skin. In this blog, I focus on the benefits of these molecules in helping to repair epidermal barrier function.
A number of diseases and conditions of the skin involve epidermal barrier dysfunction. For example, eczema is a multifactorial, heterogeneous disease associated with epidermal barrier disruption and intense systemic inflammation of the skin. Our previous work has found that S2RM attenuates the symptoms of eczema, including atopic dermatitis (AD). Studies of the mechanisms of action of the molecules present in S2RM suggest that these molecules effectively restore epidermal barrier functions in AD by facilitating the synthesis of ceramides, and creating a thicker epidermis.
hASCs as well as human dermal fibroblasts (HNDF) have a positive impact on keratinocytes proliferation, stemness maintenance, and adhesiveness to membranes via paracrine involvement when co-cultured using the collagen. This means the keratinocytes, largely responsible for building the epidermal barrier, are maintained in a younger and healthier state by the stem cells (hASCs and HNDF) that are releasing molecules into the epidermis from their location in the dermis.
These functions, along with the many other functions of the hASCs and HNDF including modulating immune function into an anti-inflammatory, pro-repair state, important to all epithelial tissues, are critical to good skin health.
The molecules released by adipose mesenchymal stem cells (ADSC) are known to bring skin cells out of senescence, and the mechanism of action is twofold: 1. the molecules released from ADSC contain SIRT1, and 2. the molecules released from ADSC increase SIRT1 expression in target cells. These are two of the many mechanisms of action underlying the ability of NeoGenesis‘ S2RM technology to rapidly and sustainably reverse and prevent the signs and symptoms of skin aging.
Longevity is a hot topic in the popular press, and the topic has now hit skincare. This is part of the “scientification” of skincare in the popular press that has arisen over the last few years. The trend has an upside and a downside. Learning about ingredients and how they work in the skin is important. The better informed we are, the better we can take care of our skin. The downside, is that non-scientists, including many practicing dermatologist, who have neither been trained as scientists, nor trained to analyze scientific studies, often proffer erroneous information about skin care in the popular press. For example, in my 2020 publication, in the section called “Example of Misinformation in Skin Care Marketing.” I describe how a practicing dermatologist in Miami makes many mistakes in describing skin care ingredients in her various popular press articles, including articles in a large newspaper.
Also, reading a Bloomberg article on what dermatologist think about anti-aging skin care products, I was once again shown an example of how misinformed are some practicing dermatologist. One dermatologist was saying not to use products that contain antimicrobial preservatives, but when looking at the products she has for sale on her website, guess what – many of the products she sells online contain an antimicrobial preservative. Looking at her blog, she talks a lot about using sunscreen – an important topic. But she misinforms the reader by saying that mineral sunscreens reflect light and UV. That’s incorrect because mineral sunscreens predominantly absorb the UV, not reflect it. I didn’t read anymore because I dislike misinformation – I’ll stick to reading informed articles from professors of dermatology, including scientists and physicians, who inform us based on scientific and clinical evidence.
Let’s look at what’s being said about longevity of the skin in the popular media, and have a brief look at some of the science in the scientific literature (PubMed, peer-reviewed journal articles).
Longevity in Skincare
As Jeannette Neumann in Bloomberg states:
In the same article, Neumann goes on to tell us that:
Key to the new product ate sirtuins. So what are sirtuins and what do they do? Sirtuins are a family of signaling proteins involved in metabolic regulation. They are ancient proteins in animal evolution and appear to possess a highly conserved molecular structure throughout all kingdoms of life. They are everywhere in lifeforms. And guess what the scientific evidence suggests: NeoGenesis not only has SIRT1 activators in our S2RM technology, but we also have the SIRT1 protein itself. We’ve had S2RM on the market for over 13 years as a topical product. It’s one of the reasons our products work so well.
Here’s a little more on sirtuins and how they’re activated. SIRT1 is a cellular defense protein that ensures survival by controlling metabolism when there is not enough energy supply to cells. SIRT1 is an important molecule in the control of redox states, apoptosis, and a number of life-extending mechanisms. By changing SIRT1 expression, a number of substances and factors can control the level of SIRT1 protein. Naturally occurring molecules that increase SIRT1 expression include, resveratrol, quercetin, fisetin, curcumin, and berberine. SIRT1 protein expression declines as a we age, and SIRT1 expression decreases with age in mice. SIRT1 has been referred to as a longevity-associated protein that could be used as a potential therapeutic target for extending human healthspan, and it is currently under investigation in the battle against cognitive decline, neurodegenerative diseases, and aging. SIRT1 has been reported to negatively regulate the expression of a number of inflammatory senescence-associated secretory phenotype (SASP) factors, including the SASP factor. SIRT1 produces neuronal protection in neurodegenerative disorders and memory impairment, and is crucial for synaptic plasticity and memory retention in neurons. Numerous studies have shown that p53 and p21 have a role in the control of the cell cycle, DNA repair, apoptosis, and other critical biological processes. Cell cycle arrest results from the activation of p53 and p21, which are responsible for replicative and stress-related senescence in cells. SIRT1 acts on p53 by deacetylating it, which negatively regulates p53’s transcriptional activity, essentially suppressing its function as a tumor suppressor and inhibiting apoptosis induced by stress or DNA damage. In other words, SIRT1 “dampens down” the activity of p53 by removing acetyl groups from it.
Senescent cells release a range of inflammatory proteins, such as SASP, which causes low-grade chronic inflammation and accelerates senescence. Loss of the key anti-aging molecule SIRT1 may be important for accelerating aging. Zhang et al (2023) found that aged mice displayed upregulation of senescence-related signals such p53 and p21 and downregulation of SIRT1 in the hippocampus. These abnormalities were reversed by the molecules released from mesenchymal stem cells (MSCs).
In our skin, fibroblasts are long-lived cells that are subject to much damage over the years. They can become senescent and pro-inflammatory. Studies have found that SIRT1 can protect human fibroblasts from senescence by promoting telomerase reverse transcriptase transcription (Yamashita et al, 2012). Further, Yuan et al (2012) found that SIRT1 improved the senescence of young MSCs during in vitro subculturing. In other words, SIRT1 protects young cells from stressors, such as oxidative stress, and keeps them healthy and from becoming pro-inflammatory senescent cell types.
As you can see from these studies, it’s not just about anti-aging, it’s about promoting longevity in the first place. We do both at NeoGenesis with our S2RM technology.
Stem cells in the skin are cells that self-renew themselves, so that they are always present in the skin. While stem cells in the skin can generate other cell types, their most important function is to continuously release molecules into the skin. Many types of molecules are released into the skin by the stem cells, the function of which is to maintain and heal the skin throughout our lives.
NeoGenesis’ S2RM technology uses all the different molecules from stem cells derived from the skin, instead of just one or a couple of molecules. S2RM technology therefore targets multiple pathways underlying a disease or condition, not just one or a few pathways as used in previous therapeutic designs. The condition, for example, can be aging, where the pathways in the skin are not working as well as they once did when the skin was young. The multiple molecules renormalize the multiple pathways and thus renormalize the physiology of the skin. For aging skin, this means the pathways are now working more like they did when we were younger. Simply put, diseases and conditions of the skin have many unique abnormal pathways that underlie the condition, and each unique pathway must be renormalized using many molecule types, each of which acts at one of the many abnormal pathways underlying the disease or condition.
Specifically, NeoGenesis uses proprietary and patented adult stem cell released molecules in its safe and effective core technology. The molecules are released, not extracted, from 3 or more types of adult stem cells derived from the skin to make our products. Using released, not extracted, molecules assures that the molecules are fully formed in their natural state and therefore effective, and naturally packaged into a protection and penetration liposome-like structure called the exosome. The exosome is like a tiny capsule, such as that used to encapsulate drugs. However, unlike the capsule, mother nature has designed the exosome to be smart. It has special structures that allow it to easily penetrate the skin and deliver the molecules where they are needed. Further, we don’t use immortalized cells that may secrete pro-oncogenic signals in their exosomes, and may also produce exosomes with an altered content, rendering them less efficacious.
Adult stem cells are partially differentiated stem cells, not embryonic stem cells. This means that the adult stem cells used by NG are more mature than embryonic stem cells, which are cells that can make any cell in the body. The adult stem cells are lineage restricted, meaning that the stem cells we use that are derived from the skin only make skin cells. Skin specific adult stem cells developed in the skin to specifically and effectively maintain and heal the skin. Because adult stem cells are tissue specific, stem cells derived from the skin work better than other types of stem cells from other parts of the body in their effectiveness to maintain and heal the skin. For example, adult stem cells derived from bone marrow don’t work well in the skin.
Key to how adult stem cells work before they differentiate into mature skin cell types is that the adult stem cells reside in the skin to maintain and heal the skin, doing so by releasing building block molecules such as collagen and laminin, and instruction set molecules, such as HAPLN-1, that signal the building block molecules how to organize. Molecules, such as HAPLN-1, decrease in concentration as we age, and as a result diseases, such as melanoma, will occur with a greater probability. From the work of Dr. Ashani T. Weeraratna, Ph.D. at Johns Hopkins, we know that supplying HAPLN-1 to aged skin can reverse this effect, and renormalize the matrix and lymphatic system in the aged skin. As she has pointed out, normal matrix in the skin is vital to good health and keeping skin cancer at bay. This follows the pioneering work by Dr. Mina Bissell, Ph.D. at Berkeley, who taught us all how critical the matrix is to cancer formation, and as I have pointed out, to many other diseases.
The NeoGenesis S2RM technology is a combination of adult stem cells of different ages where younger adult stem cells are used to make the building block molecules for scar-free healing, and slightly older stem cells make the instruction set molecules so that normal, adult skin architecture is maintained or reformed after injury. The molecules in S2RM also include those that calm inflammation and help to reset our skin’s immune system to help repair the skin. Other molecule types are present that repair damaged proteins in the skin, while other molecules prevent and repair damage to protein, lipids, and DNA.
Because we use multiple skin stem cell types, from which we collect all the molecules released, NeoGenesis’ S2RM is the most advanced skin technology available in today’s skin care market.