In a recent trial (Gupta et al, 2023), the blood pressure–lowering effect of dietary sodium reduction was comparable with a commonly used first-line antihypertensive medication. Salt in the diet is associated with chronic kidney disease. Sodium also accumulates in the skin, inducing inflammation and eczema, so feel better and look better by cutting the sodium intake that is way too high in most people.
Many factors can influence health, including that of the skin. I’ll discuss salt here, but other factors such as dairy play a big role too – both for cardiovascular health, and skin health. For example, the induction of antibodies (IgE) by the consumption of dairy can lead to cardiovascular disease and death. And dairy, loaded with antigens such as lactose, whey, and casein (even found in mothers milk because of dairy consumption by mom) can be destructive to the skin, even causing cancer.
As Gupta et al (2023) discovered, dietary sodium reduction significantly lowered blood pressure (BP) in the majority of middle-aged to elderly adults they studied. The decline in BP of those who went from a high- to low-sodium diet was independent of hypertension status and antihypertensive medication use, and was consistent across subgroups. Needless to say, reducing sodium intake did not result in adverse events.
Sodium is an essential mineral and osmolyte for the human body. It is the major cation in the extracellular fluid and as such plays a crucial role in homeostatic processes such as regulation of blood volume, osmolarity, and blood pressure. Therefore, sodium plasma concentration is maintained within a relatively narrow range of around 140 mmol/l. The sodium concentration in the interstitial space (the space in between our cells) can be much higher. We consume just the right amount of sodium when we eat a plant based diet without added sodium. If we eat too much sodium, that excessive salt intake may induce several adverse effects, causing microvascular endothelial inflammation, anatomical remodeling, and functional abnormalities, even in normotensive subjects (those with normal blood pressure). More recent studies have shown that changes in sodium plasma levels not only exert their effects on small resistance arteries, but may also affect the function and structure of large elastic arteries. The issue of salt-sensitivity, which refers to individual susceptibility in terms of BP variations following changes in dietary salt intake, has also been recently debated in its pathophysiological mechanisms and clinical implications.
Excess sodium is also stored in the skin. In the skin microenvironment, higher sodium concentrations enhance macrophage function, potentially leading to innate immune system-based inflammation. Several studies have provided significant evidence that an elevated sodium concentration has an immunomodulating effect by augmenting proinflammatory and antimicrobial macrophage function as well as T-cell activation. And now we know that sodium has accumulated to high levels in the skin of psoriasis patients (Maifeld et al, 2021). Psoriasis is an inflammatory skin condition, and restricting salt in your diet will help to reduce that inflammation. Same for eczema. Reduce the salt because, for one factor, salt promotes the growth of a bad bacteria called staph aureus which is found in patients who have bad flare ups of eczema. With high salt, the skin is unable to repair itself – it’s in a constant state of inflammation.
Cut the salt and your immune system will operate more normally. It requires time to adjust your taste to the low sodium diet – most of us are addicted to salt. But in time, you lose the addiction, and actually begin to better taste all of the other flavors in your food that were masked by the salt. Bon appetite, Pas de sel!
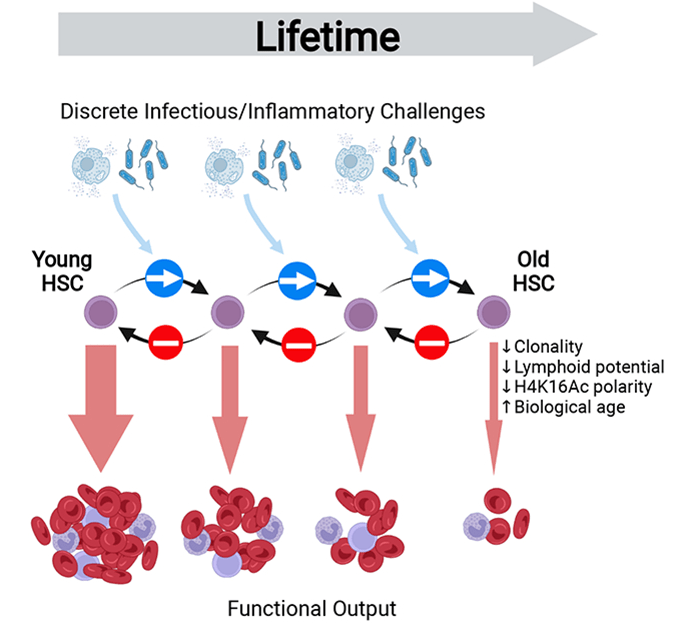
Early and mid-life inflammation ia a mediator of lifelong defects in tissue maintenance and regeneration due to the inflammation aging the stem cells.Inflammation damages the extracellular matrix, DNA, and epigenetic mechanisms, all of which contribute to aging and age-related diseases.
A schematic of stem cell inflammaging (from Bogeska et al, 2022)
Inflammaging, defined as an age-related increase in the levels of pro-inflammatory markers in blood and tissues, is a strong risk factor for multiple diseases that are highly prevalent, and frequent causes of disabilities in elderly individuals but are pathophysiologically uncorrelated, i.e., everything from cancer, to skin diseases, to heart disease, and neurodegeneration. And remember, as I’ve discussed in previous blogs, inflammation in the skin can can lead to systemic inflammation.
Inflammation can wreak havoc on the body, including the skin, through a number of key mechanisms. Let’s have a look at how inflammation can damage tissue, such as by degrading the extracellular matrix, and can damage cells at the molecular level through genetic and epigenetic mechanisms. Genetic refers to how damage occurs to the DNA, and epigenetic refers to how damage occurs “above” the DNA, such as the mechanisms that control the expression of DNA – i.e., affecting how the DNA makes RNA and proteins. Inflammation can also cause misfolding in proteins, resulting in a number of dysfunctional pathways in the body, including the control of epigenetics such as protein-based epigenetics. You read that right – proteins can be inherited and dysfunctional proteins in an adult can be inherited as dysfunctional proteins in the offspring. That’s one reason why genetics and heredity don’t mean the same thing.
Inflammaging is a process induced by chronic inflammatory cytokine signaling that promotes accelerated damage to the extracellular matrix (ECM), stem-cell aging, and precancer stem-cell generation. Multiple different sterile and infection-associated inflammatory stimuli have been shown to provoke primitive stem cells (HSCs) to exit their long-term quiescent state and enter into active proliferation. In other words, inflammation, whether it is sterile inflammation or infection-related inflammation, drives stem cells into a state where they multiply. Therefore, chronic inflammation will induce the constant multiplication of stem cells. And every time a cell multiplies itself, mutations and consequent aging processes will occur. As I’ve said before, one of the most dangerous things a cell can do is to multiply itself.
As scientists have recently published, their work demonstrates that inflammatory stimuli can provoke a long-lasting inhibitory effect on tissue regeneration that extends far beyond the duration of the original inflammatory event, via the progressive and irreversible attrition of the functional stem cell pool. They argue that prophylactic anti-inflammatory interventions may effectively delay or prevent the evolution of age-associated pathologies, but that such treatments may hold limited capacity to rejuvenate an already aged stem cell system.
In other words, it is important to reduce inflammation even during our younger years, not just during our aged period, in order to reduce stem cell aging processes. This means eating a plant-forward diet, full of lots of fruits and vegetables, as well as using sunscreen during long sun exposures, as well as using skin products that are not inflammatory – rather using skin care products that reduce inflammation and those that help to maintain or build the skin’s barrier function.
Allergic diseases affect millions of people worldwide, and are on the rise. An increase in the prevalence of these diseases has been associated with alterations in the gut microbiome, i.e., the microorganisms within the gastrointestinal tract. Maturation of the infant immune system and gut microbiota occur in parallel; thus, the normal development of the microbiome likely determines tolerant immune programming in the infant. Antigens are substances that can produce an immune response, and tolerant immune programming is a mechanism of immune tolerance where the self-antigen is protected from the immune system’s destructive response. Thus the immune system is programmed to be destructive against non-self-antigens (bacteria and viruses contain non-delf antigens, for example), but not self antigens.
A new study reported that a trend in maturation alteration is characterized by depletions in the bacterial species A. hadrus, F. saccharivorans, E. hallii, and B. wexlerae in participants who later developed allergic diseases, as well as enrichments in E. lenta, C. innocuum, E. faecalis, E. coli, and T. nexilis in these participants. The depleted bacterial populations are known short-chain fatty acid (SCFA) producers, notably the butyrate producers A. hadrus, E. hallii, and F. saccharivorans and the acetate producer B. wexlerae; SCFAs are metabolites that mediate well-defined host benefits within the gut. The authors also reported a depletion of butyrate in allergy-prone participants and significant associations between A. hadrus and F. saccharivorans respective relative abundance and butyrate concentration. This strengthens the postulation that the production of butyrate and its effect on immune cells is a mode by which optimal immune modulation occurs during early life. In contrast, species enriched in allergy-prone participants have been linked to pathogenic activity and poor health outcomes, with many of these microbiome features associating with metabolites enriched within these same participants.
Most diseases are consequence of our exposome, and not hereditary genetic factors. Our exposome greatly affects our microbiome. Established primarily during infancy, the developing microbiota’s initial expansion and fluctuation are particularly sensitive to external influences before reaching a more stable community. Sensitivity of the microbiome is most pronounced during infancy, and abnormal exposures, such as that in a hospital setting, especially during a C-section, that can drastically alter the microbiome. The number of C-Sections in 2015 doubled in comparison to those registered in 2000, and jurisdictions such as California have instituted programs to stop the medical practice of performing unneeded C-sections. Indeed, many risk factors for allergic diseases, including mode of delivery, diet, urban living, and antibiotic exposure (such as the overprescribed broad spectrum antibiotic Amoxicillin), also influence early microbiota membership and structure. Note: the broad spectrum antibiotics are particularly harmful because the drug kills so many beneficial types of bacteria. While this maturation process usually coincides with the development of healthy immune tolerance, allergic sensitization can emerge in many children because of their exposome during the same period as the microbiota is being established.
Overall, the authors compared 1115 children with asthma, allergic rhinitis, food allergy, or Eczema (atopic dermatitis) to a rigorously defined, non-allergic comparator group. They described detailed underpinnings driving this decrease in gut microbiome maturation, encompassed within the alteration of a core group of bacterial species, functional pathways (i.e., potential intestinal mucous integrity breakdown, elevated oxidative stress levels, and subsequently oxidized monosaccharides, and diminished secondary fermentation), and metabolic imbalance i.e., elevated trace amines that can be involved in inflammation and neural function, and associated with reduced microbiota-maturation age and elevated risk of allergy.
Bottom line, the infant exposome is critical for the development of a normal microbiome and a life without allergy and skin conditions without Eczema.
Professor Doctor Andreas Beyer, Ph.D., at the University of Cologne, Institute for Genetics in Germany, along with his research team has discovered that as we age, a critical process in our cells, called gene transcription, speeds up. This process involves making a copy of a specific DNA strand into the form of RNA. When the process occurs too fast, more errors are made. The RNA is then used for a number of things, including making the backbone of proteins. Posttranslational modifications then finish the making of proteins.If the protein’s backbone is error ridden, the protein loses function. Likewise, posttranslational modification (PTM) depends on other proteins, and if they are error ridden, then error ridden PTM will also lead to dysfunctional proteins.
What does this mean for our health? Dr. Beyer says, for example, “Our study is saying that, for instance, having a healthy diet or, this caloric restriction intervention, would improve the quality of the transcription of the RNA production in the cell. And this would then have beneficial effects for the cells in the long run.” The evidence for his statement; mice and worms following a low-calorie diet were assessed to gauge the impact on cell transcription during the aging process. In both scenarios, transcription’s pace was observed to be more measured, resulting in fewer errors.
To validate their experiment’s applicability to humans, they conducted assessments using blood samples from both young and elderly humans. Prof. Dr. Argyris Papantonis, Ph.D., at the University of Gottingen in Germany, one of the principal investigators, remarked, “And when we compared the young cells to the very old cells, in vitro, we got exactly the same results.”
Skin aging is characterized by the accumulation of macromolecular and molecular damage within cells, impaired ability of stem and progenitor cells to promote tissue regeneration, and restore the loss of normal physiology. Chronological aging and photo-aging are two processes of skin aging that although related, have different clinical manifestations and pathogenesis. Chronological aging appears as we age and is affected by factors such as ethnicity, individual epigenetics and exposome, and skin site. It is mainly characterized by dry skin, dullness, lack of elasticity, sagging, discoloration, and fine wrinkles. Histological features include epidermal atrophy, reduction in the number of dermal fibroblasts and collagen fibers, slackening, thinness, and functional disorganization of the cells and matrix. The primary causes are: first, the stem cell dysfunction of keratinocytes, decreased regenerative ability of stem cells in the basal layer of the epidermis leading to a decline in skin renewal and repair ability, ultimately causing aging, and second, due to the accumulation of damage and aging skin dysfunction, fibroblasts lose the ability to reshape the extracellular matrix or have a reduced ability to synthesize and secrete collagen or viscous proteins. Third, aging fibroblasts alter intracellular homeostasis through certain paracrine mechanisms Now we know an important basis for these aging associated deficits is an increase in the speed of making transcripts (RNA made from DNA), and the resulting dysfunction of proteins.
As I have written, proteins being affected by our exposome is the largest factor in diseases, including cancer. A big portion of your exposome is diet. So eat well and ignore David Sinclair, your processing of transcripts in the skin will be renormalized..
In the land of where some people will do nearly anything for money, a company is selling “human platelet extract” as a topical cosmetic product for daily use on normal skin. Can you say, “Gee, let’s clot our skin’s blood supply, induce inflammation, and induce cancer at the same time?”Yes, extended use of a platelet extract product is likely carcinogenic (Carr et al, 2014; Sabrkhany et al, 2021). To be clear, platelet lysate (extract) triggers an inflammatory response in stem cells in the skin and induces the secretion of factors maintaining immune cells (macrophages) in a proinflammatory state thus enhancing inflammation(Ulivi et al, 2014), and long term inflammation is dangerous.
First, platelet extract does not contain exosomes as some are claiming. The company Plated uses the term “Renewosome”” to fool people. It’s marketing hype that the hysterical mass media has been repeating. They even put a trademark after this silly name. Lol. Platelet-derived exosomes (PLT-Exos) are the main subtype of extracellular vesiclessecretedby platelets, which carry proteins, nucleotides, lipids, and other substances to acceptor cells, playing an important role in intercellular communication.” Notice the term “secreted.” Exosomes are actively secreted from living platelets, and an extraction process of platelets will not yield any exosomes. None. I introduced the concept of and actual products containing exosomes to skin care over a decade ago. Many people criticized me at the time, and never bothered to read my peer-reviewed work on the subject, including my scientific book on the subject. But over a decade later following my introduction of exosomes to skin care, the word is out and people are making false claims to have exosomes in their products. Again, exosomes must be released (secreted) and cannot be collected through cellular extraction processes.
BTW, if you want to buy some human platelet extract (lysate is the scientific term for extract), here’s the source:
You can also purchase the platelet extract without fibrinogen. The company has removed the fibrinogen to reduce clotting because fibrinogen is one of the clotting factors.
So, what are platelets? Platelets are anucleated red blood cells that circulate in blood. They are small because they’re anucleated and can therefore squeeze into small places. Platelets are called into action when a wound occurs and blood is spewing. Their job is to close the wound fast by clotting to stop blood leakage, and by inducing high rates of cellular proliferation and inducing an inflammatory response to fight infection. Thus, quoting from Scherlinger et al (2023) in a Nature review article, “platelets produce soluble factors and directly interact with immune cells, thereby promoting an inflammatory phenotype. Furthermore, platelets participate in tissue injury and promote abnormal tissue healing, leading to fibrosis.” Inflammation, fibrosis, abnormal tissue healing with an abnormal matrix, and proliferation are hallmarks of cancer. Tumors are wounds that don’t heal, and applying platelet extract on your face mimics a wound that doesn’t heal. Platelets don’t live long in humans, about 7-10 days, nor would you want them to. They’ve evolved to flux into an area rapidly, secrete all of their inflammatory, clotting, and proliferative factors, close the wound, and then die before before they cause too much damage. If the platelets didn’t die, but instead stayed around for a long time secreting their inflammatory, clotting, and proliferative factors, it would be similar to applying platelet extract to your skin on daily basis. Chronic inflammation, clotting and fibrosis with tumorigenesis would result.
If we consider platelet rich plasma (PRP), a less concentrated form of platelet extract, an inflammatory response in fibroblasts is induced that leads to the formation of ROS (reactive oxygen species) and activation of oxidative stress pathways. It does not promote regeneration. Recent studies have found, “Treatment with PRP increased reticular dermis thickness with a fibrotic aspect. In the long term, the presence of inflammation and microangiopathy caused by PRP injection could lead to trophic alteration of the skin and the precocious aging process.” In other words, platelets cause fibrosis and advanced aging of the skin. Why someone would want to use platelet extract on their skin is beyond me.
According to epidemiologists, “A growing body of laboratory research has shown the direct involvement of platelets with cancer.: Cancer follows a high platelet count. Signaling by platelet-derived growth factors (PDGFs) and their receptors (PDGFRs) is commonly observed in epithelial cancers, where it triggers stromal recruitment and may be involved in epithelial–mesenchymal transition, thereby affecting tumor growth, angiogenesis, invasion, and metastasis. In other words, the extract of platelets will be high in PDGF and when applied daily will enhance the probability of cancer.
Recent studies have found that over-active PDGF signaling is implicated in several types of human malignancies, in one way by promoting proliferation, survival and invasion of tumour cells directly, and in another way by changing the tumor stroma (matrix) in a manner that promotes tumorigenesis. If we look at a product called Regranex, which is a topical product containing 0.01% PDGF, the label includes a warning, “Malignancies distant from the site of application have occurred in REGRANEX users in a clinical study and in postmarketing use.” Thus, using a platelet extract, loaded with PDGF, on a daily basis may be asking for trouble, specifically tumorigenesis.
Let’s look at the ingredients of the platelet extract product used in a “clinical study” of the platelet extract product (from their website):
Question – If the “human platelet extract” is so good, why do they need to include all of those other actives?
Answer- because the platelet extract doesn’t work well on its own. At NeoGenesis, we don’t have to add anything to our S2RM adult stem cell-based technology containing exosomes because it really works.
Let’s look at a study published by the company selling platelet extract. The study is:
This study is for short term results in treated skin, not long term results in normal skin. The study suffers from a poor experimental design, conflicts of interest, and the results are underwhelming,
First, the study was not conducted at Mayo Clinic as some people have said in social media. Rather the study was performed for payment from the company to a plastic surgeon named Steve Dyan, and the authors included those employed by the company. So Steve Dyan put his name on the paper for money – this is common, and is called ghostwriting. This is where a physician puts their name on a paper when others have done the work. He was paid to put his name on this published paper. This is a conflict of interest, and is one of the reasons why most medical research and clinical trials cannot be believed.
Look at the study design, and find the problem with the design:
Treatment Group – Before Procedure: “A 7-day pre-procedure facial skincare regimen for subjects randomized to the HPE treatment group included Cetaphil cleanser (or equivalent) twice daily morning and evening, with application of HPE once daily, and EltaMD (Colgate-Palmolive, New York, NY) UV Daily Broad-Spectrum SPF 40 (or equivalent) in the morning, with reapplication throughout the day as needed.” Treatment Group – Post-Procedure:
“Post-procedure skincare (until the skin was fully healed at 7–10 days) in the treatment group included application of HPE three times daily (morning, mid-day, and before bedtime) followed by Vanicream (PSI, Rochester, MN) Moisturizing Ointment as needed for dryness, applied 15 min after HPE CALM. Post-healing when were they [sic] determined “healed” skincare in the HPE treatment group included Cetaphil (Galderma, Fort Worth, TX) cleanser twice daily, application of HPE three times daily, sunblock, and Vanicream.”
Control Group: “Post-procedure skincare in the control group (until the skin was fully healed) included application of silicone gel twice daily and application of Vanicream Moisturizing Ointment as needed for dryness. After complete healing, the control group used Cetaphil cleanser twice daily and application of sunblock.”
Do you see the problems?
A proper study design will make the control and experimental groups the same except for the one variable, which is the test product.
Did the study do this?
No, the treatment group received extra care in the form of 7-day pre-procedure care.
Are the results convincing?
No, look at the pictures and the data – the improvement is minimal if at all.
Why didn’t the study use an active comparator? Basically this is a study of platelet extract versus doing nothing. A good study would have compared the platelet extract to something that is known to improve post-procedure healing, something like, say, NeoGenesis Recovery. The company decided to compare their product to doing nothing, and even when compared to doing nothing, the results are poor.
I could have formulated a product using platelet extract years ago, but decided not to because it is not good for the skin (inflammation and fibrosis) and is dangerous (tumorigenesis). So, if you want clotted blood vessels in your skin, tumorigenesis, fibrosis, and inflammation, go ahead and do as some company wants you to do, apply platelet extract to your face daily. Halloween is coming in a couple of months, and if you start now, you won’t need a costume.
Mesenchymal Stem Cells and their Progenitor Cells (Fibroblasts) Derived from Skin are Superior to Bone Marrow Derived Mesenchymal Stem Cells
When addressing safety and efficacy concerns of stem cells, we must consider tissue-specific stem cells. Choosing the appropriate stem cell type to match the condition to be treated is critical not only to efficacy, but most importantly, safety of the therapeutic. Beyond the genetic and epigenetic factors that influence stem cell phenotype as embryonic stem cells differentiate into somatic stem cells, the immediate niche of the stem cell will have profound influence on the cell’s phenotype. Therefore, the appropriate use of adipose derived mesenchymal stem cells (ADSCs), and their related progenitor cells from the skin, fibroblasts, is optimal for skin care compared to bone marrow mesenchymal stem cells (BMSCs)
Let’s consider some of the problems BMSCs pose for developing skin care products. The complexity of the bone marrow (BM) niche can lead to many stem cell phenotypes, whether we consider hematopoietic stem cells (HSCs) or bone marrow mesenchymal stem cells (BMSCs). Here I will discuss the properties of BMSCs, not HSCs. Because of the complexity, many BMSC phenotypes exist, including disease causing phenotypes that are varied and hard to distinguish – a part of the problem in using BMSC for therapeutic development. This complication, unlike that for ADSCS, includes recirculated cells, particularly recirculated cancer cells. Once a tumor cell disseminates into the BM, the cancer cell often displays phenotypic characteristics of BMSCs rendering cancer cells difficult to distinguish from BMSCs. BM is a site of BMSCs that may differentiate into HSCs and recirculating blood cells that may differentiate into BMSCs [see Cardenas et al; Tondreau et al]. BMSCs are also found outside of the niche in peripheral blood and home into sites of injury and cancer tissue where they are educated into becoming a pro-cancerous phenotype. Recirculated melanoma and myelogenous leukemia cells in BM interact with BMSCs to change the phenotype of the BMSC to one that is cancer promoting by enhancing their proliferation, migration, and invasion and altering the production of proteins involved in the regulation of the cell cycle. Indeed, melanoma tumor cells start to disseminate to BM during the initial steps of tumor development. In breast cancer patients, detection of recirculated cancer cells that disseminated in BM predicts recurrence of the cancer. Cancer cells can fuse with BMSCs and change their phenotype, or release exosomes to change the phenotype of BMSCs to cancer promoting. Indeed breast tumor cells fuse spontaneously with bone marrow mesenchymal stem cells. This fusion may facilitate the exchange of cellular material from the cancer cell to the BMSC rendering the fused cell more oncogenic. Further, others have found the same result of this fusion and exchange of cellular material, which has been found to increase metastasis. For example, Li et al found that human hepatocellular carcinoma cells with a low metastatic potential exhibit a significantly increased metastatic potential following fusion with BMSCs in vitro and in xenograft studies. This means that the BMSCs and their molecules/exosomes, having been conditioned by tumor cells, were found to increase the probability of cancer in human patients. The various phenotypes of BMSCs, including the cancerous phenotypes are difficult to distinguish. In contrast, even ADSCs derived from cancer patients have been found to be safe for therapeutic development.
One of many reasons why ADSCs are preferred compared to BMSCs is that ADSCs express a low level of major histocompatibility complex (MHC) class I molecules and do not express MHC class II and costimulatory molecules. Even the exosomes of BMSCs express MHC class II proteins. These problems in BMSCs are amplified when using donor, allogeneic BMSCs that have been replicated many times, essentially aging the cells, during expansion to develop the therapeutic. This is in contradistinction to ADSCs. Critically, when comparing experimental data of BMSCs to ADSCs from the same human donor, “ADSCs have a “younger” phenotype,” according to stem cell scientists. Indeed, Burrow et al found that BMSCs have, among other negative attributes compared to ADSCs, an increased level of senescence compared to matched ADSCs. Senescent cells develop the senescence-associated secretory phenotype (SASP), a pro-inflammatory set of molecules where the local tissue effects of a SASP or specific SASP components have been found to be involved in a wide variety of age-related pathologiesin vivo such as hyperplastic diseases, including cancer. Whereas the use of BMSC transplants has a history of medical adverse events, including the induction of cancer in the recipient (Maguire, 2019), fat grafting, along with its constituent ADSCs, have a long history of safety in medical procedures dating back to 1893 when the German surgeon Gustav Neuber transplanted adipose tissue from the arm to the orbit of the eye in an autologous procedure to fill the depressed space resulting from a postinfectious scar. Fat grafting’s long history of being safe, regardless of the harvesting techniques used in patients, has been recently reviewed by physician-scientists at Baylor College of Medicine. Furthermore, physician-scientists at Stanford University School of Medicine have recently reviewed the safety and efficacy of using ADSCs to augment the outcomes of autologous fat transfers. Scientists have found that ADSCs and fat grafting for treating breast cancer-related lymphedema is safe and efficacious during a one year follow-on, where patient-reported outcomes improved significantly with time. In a randomized, comparator-controlled, single-blind, parallel-group, multicenter study in which patients with diabetic foot ulcers were recruited consecutively from four centers, ADSCs in a hydrogel was compared to hydrogel control. Complete wound closure was achieved for 73% in the treatment group and 47% in the control group at week 8. Complete wound closure was achieved for 82% in the treatment group and 53% in the control group at week 12. The Kaplan–Meier (a non-parametric statistic used for small samples or for data without a normal distribution) median times to complete closure were 28.5 and 63.0 days for the treatment group and the control group, respectively. Treatment of patients undergoing radiotherapy with adult ADSCs from lipoaspirate were followed for 31 months and patients with “otherwise untreatable patients exhibiting initial irreversible functional damage” were found to have systematic improvement or remission of symptoms in all of those evaluated. In animal models with a full thickness skin wound, administration of ADSCs, either intravenously, intramuscularly, or topically, accelerates wound healing, with more rapid reepithelialization and increased granulation tissue formation, and topically applied the ADSCs improved skin wound healing by reducing inflammation through the induction of macrophage polarization from a pro-inflammatory (M1) to a pro-repair (M2) phenotype.
All in all, companies using BMSCs to develop their skin care products demonstrates a profound ignorance of the related science. Incompetence, and a greedy, lazy approach to serving the skin care market is demonstrated by those using bone marrow stem cells to develop skin care products that potentially damage their clients.
Stem cells in the skin are cells that self-renew themselves, so that they are always present in the skin. While stem cells in the skin can generate other cell types, their most important function is to continuously release molecules into the skin. Many types of molecules are released into the skin by the stem cells, the function of which is to maintain and heal the skin throughout our lives.
NeoGenesis’ S2RM technology uses all the different molecules from stem cells derived from the skin, instead of just one or a couple of molecules. S2RM technology therefore targets multiple pathways underlying a disease or condition, not just one or a few pathways as used in previous therapeutic designs. The condition, for example, can be aging, where the pathways in the skin are not working as well as they once did when the skin was young. The multiple molecules renormalize the multiple pathways and thus renormalize the physiology of the skin. For aging skin, this means the pathways are now working more like they did when we were younger. Simply put, diseases and conditions of the skin have many unique abnormal pathways that underlie the condition, and each unique pathway must be renormalized using many molecule types, each of which acts at one of the many abnormal pathways underlying the disease or condition.
Specifically, NeoGenesis uses proprietary and patented adult stem cell released molecules in its safe and effective core technology. The molecules are released, not extracted, from 3 or more types of adult stem cells derived from the skin to make our products. Using released, not extracted, molecules assures that the molecules are fully formed in their natural state and therefore effective, and naturally packaged into a protection and penetration liposome-like structure called the exosome. The exosome is like a tiny capsule, such as that used to encapsulate drugs. However, unlike the capsule, mother nature has designed the exosome to be smart. It has special structures that allow it to easily penetrate the skin and deliver the molecules where they are needed. Further, we don’t use immortalized cells that may secrete pro-oncogenic signals in their exosomes, and may also produce exosomes with an altered content, rendering them less efficacious.
Adult stem cells are partially differentiated stem cells, not embryonic stem cells. This means that the adult stem cells used by NG are more mature than embryonic stem cells, which are cells that can make any cell in the body. The adult stem cells are lineage restricted, meaning that the stem cells we use that are derived from the skin only make skin cells. Skin specific adult stem cells developed in the skin to specifically and effectively maintain and heal the skin. Because adult stem cells are tissue specific, stem cells derived from the skin work better than other types of stem cells from other parts of the body in their effectiveness to maintain and heal the skin. For example, adult stem cells derived from bone marrow don’t work well in the skin.
Key to how adult stem cells work before they differentiate into mature skin cell types is that the adult stem cells reside in the skin to maintain and heal the skin, doing so by releasing building block molecules such as collagen and laminin, and instruction set molecules, such as HAPLN-1, that signal the building block molecules how to organize. Molecules, such as HAPLN-1, decrease in concentration as we age, and as a result diseases, such as melanoma, will occur with a greater probability. From the work of Dr. Ashani T. Weeraratna, Ph.D. at Johns Hopkins, we know that supplying HAPLN-1 to aged skin can reverse this effect, and renormalize the matrix and lymphatic system in the aged skin. As she has pointed out, normal matrix in the skin is vital to good health and keeping skin cancer at bay. This follows the pioneering work by Dr. Mina Bissell, Ph.D. at Berkeley, who taught us all how critical the matrix is to cancer formation, and as I have pointed out, to many other diseases.
The NeoGenesis S2RM technology is a combination of adult stem cells of different ages where younger adult stem cells are used to make the building block molecules for scar-free healing, and slightly older stem cells make the instruction set molecules so that normal, adult skin architecture is maintained or reformed after injury. The molecules in S2RM also include those that calm inflammation and help to reset our skin’s immune system to help repair the skin. Other molecule types are present that repair damaged proteins in the skin, while other molecules prevent and repair damage to protein, lipids, and DNA.
Because we use multiple skin stem cell types, from which we collect all the molecules released, NeoGenesis’ S2RM is the most advanced skin technology available in today’s skin care market.
The stem cell released molecules that NeoGenesis uses in our S2RM technology is a mixture of proteins, micro-RNA and lipids that is from skin derived mesenchymal stem and progenitor cells. This technology is a new means for therapeutic development. The molecules that are released from the different stem cell types are largely packaged into exosomes. Exosomes under 150 nm in diameter do not contain DNA, whereas larger extracellular vesicles (EVs) can contain small amounts of DNA. Exosomes are made by cells in different process than the way EVs are made. As with other studies characterizing vesicles secreted from mesenchymal stem cells, we have found the size of the exosomes (small extracellular vesicles) to about 50-80nm in diameter. Again, these exosomes have not been found to contain DNA. At NeoGenesis, we also use filtration methods in the production of the S2RM that would prevent large EVs from entering our S2RM. As stated by Rani et al (2015), “the fundamental basis for MSC-EV therapeutic effects lies in their ability to transmit biological information—in the form of proteins, glycoproteins, lipids, and ribonucleic acids—from stem cells to injured cells.” This is an important part of the exosomal S2RM technology, but there is more. The S2RM is also, 1. immune modulating to bias towards tissue repair and away from inflammation, 2. supplies important building blocks for tissue repair, such as collagen, 3. many types of antioxidants to help repair and protect proteins, DNA, and lipids, and 4. supplies proteosomes to carry away damaged cells for recycling. Attributes one through four are in addition to the repair properties of the S2RM that include growth factors, and heat shock proteins to repair proteins and DNA. Important to note is that the exosomes work in concert with soluble proteins to repair tissue – it’s not just the exosomes. This is why NeoGenesis uses the exosomes and the soluble proteins (the fraction of proteins not contained in the exosomes) in our S2RM technology. – we don’t through away the good and synergistic part of what stem cells release, a fraction of the S2RM that contains many proteins, including heat shock proteins. The fraction not contained in exosomes also contains many important signaling lipids that reduce inflammation, such as PEA, and that build the extracellular matrix. And it’s also important to note the cells we use from the skin are superior in this regard, and may others ways too, than the mesenchymal stem cells from bone marrow.
Quality control, efficacy, safety, and the production of novel products is key to doing it ourselves
NeoGenesis is a vertically integrated company that formulates, manufactures, and sells skin care products, including those classified as drugs and cosmetics. We even make our own stem cell released molecules in a high level biotech facility on site. Many reasons lead NeoGenesis to formulate and manufacture our products within our own facilities. For example, when I created the S2RM technology, no one else on the planet was making such an ingredient, let alone even knew what it was. This is a new type of active ingredient that had to be developed and then scaled for commercial production. We had to do it ourselves at NeoGenesis because no one else knew how to do it. This is still the case.
Here’s another reason we don’t use contract manufacturers that’s often not considered. Having our own manufacturing facility means that our products are not cross-contaminated with chemicals that we don’t want in our products for safety and efficacy reasons. This’s what often happens when small companies employ a contract manufacturer. One company will be producing a product with, for example, parabens, which are endocrine disruptors, and those parabens will be included in a company’s products who doesn’t want them because of cross contamination. At NeoGenesis, we don’t use parabens and so there is no chance of cross contamination
Little things are important when formulating. For example, we don’t use coconut oil in our products because it’s comedogenic -it clogs pores. I’ve recently formulated a mineral sunscreen that doesn’t use coconut oil or the ingredient BOS (Butyloctyl salicylate) as do many other companies. Why? Because BOS is a salicylate. And salicylates convert back to salicylic acid when they’re metabolized in the skin and other parts of the body, making them potentially toxic, especially for pregnant women. And children shouldn’t be exposed to salicylates at any concentration. Remember, children are undergoing rapid development, and toxins can negatively perturb developmental pathways potentially leading to life-long disease. Salicylic acid is a drug regulated by the FDA. For good reason, because it is easily systemically absorbed by the body and can be toxic. Children under 2 yrs should not use it. Unfortunately common in the chemical industry is that some companies will slightly modify a compound’s structure such that the altered substance stealthily flies under the radar of overwhelmed regulators, such as the FDA. BOS is one of those ingredients.
When Neogenesis formulates and manufactures our products, we know what’s in our product. Many contract manufacturers will source the lowest cost ingredients possible, and the formulations will also be made with the profit in mind first, over quality. Some will leave out an expensive ingredient to cut their cost of manufacturing and increase their profit. Some companies have been caught adding drugs, such as steroids, to their cosmetic products without disclosing these possibly dangerous chemicals to their customers.
Another aspect of being a vertically integrated company is that we control our sales and marketing. The narrative we tell is our own, and won’t be some made-up fictious story making wild claims that aren’t true. When we sell a product to someone it is meant to be beneficial to them, and not simply to take their money. As my father always taught me, if you take someone’s money, you need to give them something of value in return. Not every product that we make and sell will be right for a particular person – at NeoGenesis we let you know what is best for your skin and what may not be useful for you.
There are a number of ethical companies in the skin care industry – chose carefully, because some, such as Cosmetic Innovations in Texas, are not.
DNA damage is at least one of the signals generated by ultraviolet radiation that stimulates pigmentation production (tanning) in human skin. Don’t damage your p53 (it’s a tumor suppressor).
The photoprotective tanning response is functionally similar to the SOS response described in bacteria. The SOS response results from DNA damage in which the cell cycle is arrested and DNA repair and adaptive mutagenesis is induced. Adaptive mutations may reflect an inducible mechanism that generates genetic variability in times of stress. Basically, it’s an ancient survival mechanism. While there are benefits, there are also negative consequences. As such, it’s best not to stress the skin with too much sunshine. As I’ve previously discussed in a review paper, small amounts of sun exposure are beneficial, including to the skin’s adaptive immune system (T-cells), but once you start tanning, the negative effects on the skin begin.
DNA damage stimulates pigmentation, at least in part, through up-regulation of tyrosinase mRNA and protein levels. Interestingly, scientists have found this response can be induced in the absence of DNA damage by treatment of melanocytic cells and intact skin with small DNA fragments, particularly thymidine dinucleotides, pTpT. Application of these DNA fragments have been found to provide a photoprotective tan to human skin cells without the harmful effects of ultraviolet radiation.
For my fellow nerds out there who like to learn about cellular and subcellular signaling pathways in the skin, here’s what happens (from Dr. Suzanne Clancy, Ph.D): Incident UV radiation on the skin causes two classes of DNA lesions: cyclobutane pyrimidine dimers (CPDs) and 6-4 photoproducts (6-4 PPs). Both of these lesions distort DNA’s structure, introducing bends or kinks and thereby impeding transcription and replication. Relatively flexible areas of the DNA double helix are most susceptible to damage. One “hot spot” for UV-induced damage is found within a commonly mutated oncogene, the p53 gene. The p53 gene is a so-called tumor suppressor gene. If damaged, tumors more easily develop.
So coverup in the sun, and/or wear a sunscreen. Before and after going out in the sun, use a topical product that contains a variety of antioxidants, including but not limited to Vitamin C, to replace the antioxidants that were degraded by the sunlight. Using an antioxidant product, such as NeoGenesis Recovery and the new Neogenesis Vitamin C/Antioxidant product that will soon be released, will help to protect and repair DNA (and proteins and lipids), and may reduce your chances of developing cancer.