There’s some bullcrap on social media promulgated by a physician who wasn’t trained as a dermatologist and lost his mecidal license, saying that low molecular weight hyaluroic acid (HA) is bad for the skin. Little could be further from the truth. Let’s explore the benefits of low molecular weight hyaluronic acid, and even HA nanoparticles. The benefits are huge.
HA is a type of glycosaminoglycan (GAG), and is found in many parts of the body, including the skin. In the skin, HA retains and evenly distributes water, thus preserving the volume of the skin and its elastic and flexible properties.. HA also plays a protective role as an inhibitor of free radicals, generated upon exposure to solar radiation. HA has been reported to be about one third of the total amount of both the dermis (±0.5 mg/g wet tissue) and the epidermis (±0.1 mg/g wet tissue. In the epidermis, the HA is metabolized and actively participates in many regulatory processes, such as cell proliferation, migration, and differentiation. In the dermis, it fills the extracellular spaces
The benefits of using topical low molecular weight hyaluronic acid (LMHA) in your skincare routine are many. Here are a few key benefits that make this ingredient a must-have in your skincare routine:
Deep Hydration: LMHA delivers moisture deep into the skin layers, ensuring that your skin remains hydrated for a longer period.
Reduced inflammation: LMHA has been found to decrease inflammatory cytokines in the skin
Improved Skin Texture: Regular use of LMHA can lead to a smoother and softer skin texture, thanks to its ability to boost collagen production.
Reduced Signs of Aging: LMHA can help minimize the appearance of fine lines and wrinkles, giving your skin a youthful glow.
Enhanced Skin Barrier: By providing deep hydration, LMHA strengthens the skin’s barrier function, protecting it from environmental stressors.
Let’s look at some of the evidence:
Hyaluronic acid nanoparticles (HA-NPs) have recently been found to exhibit significant efficacy in treating psoriasis, one of the inflammatory skin diseases (ISDs) (Lee et al, 2022). HA particles were able to penetrate deep into the skin and were hyaluronidase (HYAL) resistant. Furthermore, the HA particles exhibited receptor-mediated targeting of pro-inflammatory M1 type macrophages in inflamed skin. This macrophage-targeting ability of HA-NPs has also been observed in other inflammatory diseases such as type 2 diabetes, atherosclerosis, and IBD.
Low-molecular-weight hyaluronan (LMHA) is obtained by changing the molecular weight or modifying the functional groups of HA. In contrast to the stratum corneum impermeability of high-molecular-weight HA (1000–1400 kDa), the LMHA (20–300 kDa) has been reported to pass through the stratum corneum by Raman spectroscopy (Essendoubi et al, 2016).
Positive Effects of LMHA
Increases NMF. Low molecular weight HA and nano-particles of HA have been found to provide many benfits to the skin. For example, evidence suggests that topical application of LMHA resulted in an increase in natural moisturizing factor and promote moisturization of the stratum corneum (Hashimoto and Maeda (2021).
Increases CASP14 and stratum Corneum Formation. Proteolytic activation of CASP14 is associated with stratum corneum formation, implicating CASP14 in terminal keratinocyte differentiation and cornification When LMHA was applied topically to the 3D epidermis model, the mRNA level of CASP14 was increased, and the activity of CASP14 was increased in the stratum granulosum and stratum corneum (Hashimoto and Maeda, 2021). They found that HA of molecular weights of 10 kDa or less can penetrate deep into the stratum corneum, affecting FLG-degrading enzymes in the stratum granulosum and mucopolysaccharides in the basal layer of epidermis.
LMW-HA-induced activation of keratinocytes that is not accompanied by an inflammatory response, because no production of IL-8, TNF-α, IL-1β, or IL-6 was observed (Gariboldi et al, 2007)..
500-kDa HMW-HA protects macrophages from LPS-induced inflammation, i.e. inflammatory cytokines, through an interaction between HMW-HA/CD44 and LPS/TLR4 signals (Muto et al, 2009).
Both LMW-HA and HMW-HA have inhibitory effects on TLR-mediated macrophage inflammation, therefore HA has a high capacity to suppress TLR4-related keratinocyte inflammation (Hu et al, 2022).
Highly expressed IL-6 in psoriatic skin stimulates abnormal keratinocyte proliferation, and IL-6 inhibition by HA (Hu et al, 2022) is helpful in maintaining skin homeostasis in conditions such as psoriasis
Low MW HA inhibits Th1 mediated inflammatory immune response (Zheng et al, 2022).
Topical LMHA significantly contributes to wrinkle resuction (Pavicic et al, 2011).
LMHA influences the expression of various genes including those contributing to keratinocyte differentiation and formation of intercellular tight junction complexes without showing proinflammatory activity (Farwick et al, 2022).
LMHA can promote wound healing by accelerating epithelization through the HIF-1α/VEGF pathway (Liu et al, 2024).
LMHA, 35 kDa low molecular weight hyaluronan fragment (HA35) has been found to alleviate pain when applied subcue (Zhang et al, 2024), thus it may have similar effects when applied to the skin.
LMHA when applied with amino acids, increased fibroblast activity resulting in the production of Type III reticular collagen, as well as an increased number of blood vessels and epidermal thickness (Scarano et al, 2024).
LMHA is better than high MWHA (HMHA) in mosituring the skin of aged people (Muhammad et al, 2024).
Low molecular weight hyaluronic acid prevents oxygen free radical damage to granulation tissue during wound healing (Trabucchi et al, 2002).
LMHA inhibits inflammation through inhibition of leukocytes (Jia et al, 2023)
Butyrate conjugated forms of HA (one of the forms of HA that NeoGenesis uses) have been found to be anti-inflammatory by modulating cytokine expression and increasing lymph flow, thus preventing chronic wounds of all kinds from entering a chronic inflammatory state (Gao et al, 2019).
Summary
If you’re not using topical LMHA in your skin care routine, you’re likely to realize sub-optimal results.
NeoGenesis uses Hydroxypinacolone retinoate (HPR), a newer retinoid that is less irritating than tretinoin and has been found to be as effective in vitro at promoting collagen production. HPR is also more stable than other retinoids in the presence of sunlight and air. Unlike retinol, HPR directly binds to the retinoid receptors and is therefore more effective and less irritating than retinol. The efficacy of HPR is similar to retinoic acid. However retinoic acid (tretinoin) can cause significant irritation of the skin, and is available only by a physician’s prescription. Retinoids can provide great benefit to aging skin. In this blog, I’ll explore some of the mechanisms by which retinoids benefit both the epidermis and the dermis. (Christine Preston contributed to this blog).
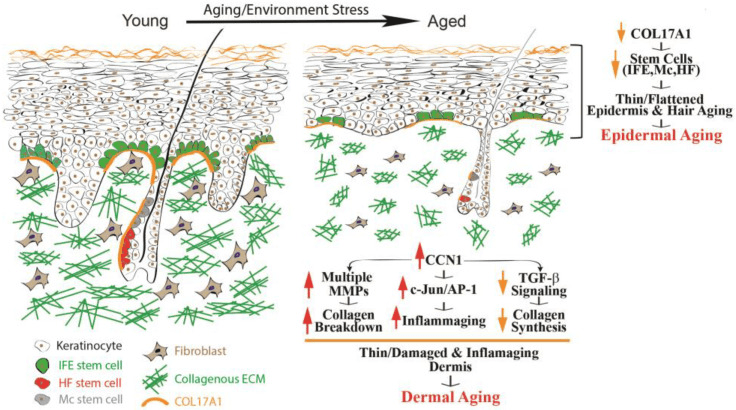
From Quan (2023)Epidermal and dermal aging of human skin. Skin aging includes the thinning of both the epidermis and dermis.
Over time, many alterations occur within the epidermis, collectively known as epidermal aging. These changes in time are characterized by the thinning of the epidermal layer and the flattening of rete ridges (as depicted in Fig 1, on the right). Rete ridges (RR) form an interdigitated surface area that reinforces cohesion between the epidermis and dermis, and this structure demonstrates plasticity, responding dynamically to stimuli such as UV irradiation. RR adapts to disruptions of its boundary during wound repair when cells lose hyper-adhesiveness, allowing the skin to appropriately remodel itself. The principal cause of epidermal aging can be traced to a reduction in the proliferation and turnover of keratinocytes, linked partially to the depletion of interfollicular epidermal (IFE) stem cells and dysfunctional Rete Ridges, leading to poor healing and thinning of the epidermis.
Collagen type, COL17A1 has been of particular interest due to its role in maintaining the homeostasis of the skin stem cells. COL17A1 is a structural element within the dermal–epidermal basement membrane, and it is synthesized by epidermal keratinocytes, not fibroblasts (Xiang et al, 2022). COL17A1 is primarily expressed in the uppermost extensions of the rete ridges area, where the niches for IFE stem cells are located. Research results have suggested a reduction in the expression of COL17A1 in human skin affected by both intrinsic and extrinsic aging factors, including human skin exposed to acute UV irradiation. The decrease in COL17A1 levels within the area specific to the rete ridges can reduce the adherence of IFE stem cells to their designated locations, leading to their removal from the skin. Consequently, the reduction of collagen protein, COL17A1, results in decreased rates of keratinocyte renewal and the development of thinner epidermal layers, the primary morphological characteristic of aging skin.
Human skin has developed two main defense mechanisms to guard against the damaging effects of UV: 1. epidermal thickening, 2. and the stimulation of melanin synthesis, however, photoprotection through increased melanogenesis is more important. As we think about retinoids and what they do for the skin, think about how retinoids help to maintain the normal structure of the skin, can actually thicken the epidermis and dermis, and how important this is for skin function and protection, including protection against UV.
Retinoids, which refer to a group of vitamin A derivatives, are among the most-extensively studied ingredients in skincare for combatting aging and enhancing the appearance of mature skin. Retinoids can stimulate collagen synthesis, inhibit MMP (Matrix metalloproteinases – too much of this activity can break-down proteinaceous tissues) activity, reduce oxidative stress, and modulate gene expression (Quan, 2023). Retinoids have exhibited efficacy in ameliorating the visual manifestations of both intrinsic and extrinsic aging, such as wrinkles, fine lines, and irregular pigmentation. The mechanisms of retinoid’s action may involve the activation of retinoic acid receptors (RARs) and retinoid X receptors (RXRs), which regulate gene transcription and cell differentiation. Retinoids may also modulate the activity of growth factors and cytokines involved in ECM turnover and inflammation. Retinoic acid (RA) is the active form of vitamin A and its precursor is called retinol (ROL). ROL can be converted into its active metabolite within human skin. When retinol is applied topically to human skin, it can penetrate the skin and undergo sequential conversion to retinaldehyde and then to retinoic acid
Skin-equivalent cultures have been used to investigate the regulatory role of retinoids in collagen homeostasis. Typically, these simplified skin constructs feature stratified and differentiated keratinocytes, representing the epidermal layer, layered atop a collagen lattice primarily comprising Type I collagen. Dermal fibroblasts are embedded within this lattice to mimic the dermal layer. When subjected to retinoic acid treatment, these skin-equivalent cultures exhibit a thickened epidermis with a substantial increase in the number of keratinocyte layers and elicit a dermal response akin to the effects observed when retinoic acid is topically applied to human skin in vivo. Consequently, skin-equivalent cultures hold significant potential as a valuable model for delving into the mechanisms by which retinoids enhance the appearance of aging skin in humans.
Increasing the Thickness of the Epidermis and the Vascularity of the Dermis in Aged Human Skin In Vivo Using Topical Retinoids: Stimulating the Growth of Epidermal Keratinocytes and Dermal Endothelial Cells
Topical application of retinoids to aged human skin in a live setting has been found to significantly enhance the thickness of the epidermis by stimulating the proliferation of epidermal keratinocytes, and increasing the number of Rete Ridges. In addition to improving epidermal thickness, topical retinoid has shown a notable increase in the proliferation of endothelial cells and blood vessels in the papillary dermis. These findings suggest that the topical application of retinoids results in the thickening of the epidermal layer and the development of fresh blood vessels within the dermis. The AP-1 transcription factor is critical to enabling the proliferation of keratinocytes in response to growth factors, cytokines, and various stimuli. The AP-1 complex consists of c-Jun and c-Fos, and it has been observed that topical retinoids significantly increases the expression of the epidermal-specific c-Jun protein, leading to a substantial increase in epidermal thickness. There is also evidence that the expression of c-Fos protein increases with retinoid treatment. These findings suggest that topical retinoids enhance the activity of the epidermal-specific c-Jun, and possibly c-Fos transcription factors, thereby stimulating the proliferation of epidermal keratinocytes in aged human skin in vivo.
Topical Retinoids Improve the Dermal ECM Microenvironment by Promoting the Production of Collagenous ECM in Aged Human Skin In Vivo
Topical retinoid treatment increases Type I collagen expression, which constitutes 80–85% of the dermal ECM, while collagen type III constitutes about 8–11%. Topical retinoid also significantly enhances the expression of fibronectin and tropoelastin. In aged human skin in vivo, topical retinoid effectively activates dermal fibroblasts, leading to the substantial production of collagenous ECM through the activation of the TGF-β/Smad pathway, which is a key regulator of ECM production. Topical retinoid administration causes a significant increase in TGF-β1 mRNA expression and a decrease in inhibitory Smad7, while other components of the TGF-β pathway remain unaffected. Additionally, topical retinoid leads to an increase in the expression of connective tissue growth factor (CTGF/CCN2), which is substantially reduced in the dermis of aged individuals and contributes to the decline in collagen production associated with aging. These findings provide evidence that topical retinoid stimulates the production of ECM by dermal fibroblasts through the upregulation of the TGF-β/CTGF pathway in aged human skin.
In addition to the upregulation of TGF-β/CTGF pathway, retinoic acid significantly reduces CCN1 gene expression in both naturally aged and photoaged human skin in vivo. CCN1 is a negative regulator of collagen homeostasis by inhibiting the TGF-β/CTGF pathway and stimulating MMPs’ induction. These data suggest that the mechanism by which topical ROL improves aged skin, through increased collagen production and inhibition of MMPs, may involve the downregulation of CCN1. Thus, retinoids are acting through multiple pathways, inhibiting some and activating others.
In aging skin, decreased vascularity and thinning of the dermis and epidermis are substantial factors contributing to skin fragility and hindered wound healing. Blood flow to the skin, the largest organ in the body, is reduced by 40% between the ages of 20 to 70 years. Topical retinoids not only enhances ECM production, but also improves the dermal microenvironment by promoting the expansion of vasculature through endothelial cell proliferation in aged human skin. An age-related reduction in cutaneous vasculature has been reported. The increased vascularity of the dermis induced by topical retinoids can improve skin blood flow and create a more-favorable microenvironment for the homeostasis of the epidermis and dermis. Further, the promotion of epidermal keratinocyte proliferation and the restoration of ECM production by topical retinoid could create a supportive environment for the growth of endothelial cells and the development of dermal blood vessels. Epidermal keratinocytes are a significant source of vascular endothelial growth factor (VEGF), a powerful factor in promoting angiogenesis. Furthermore, increased production of dermal ECM has been demonstrated to stimulate the proliferation of endothelial cells. As a result, the augmented dermal vascularity facilitated by retinoids may have a significant impact on the homeostasis of both the epidermis and dermis.
Hydroxypinacolone Retinoate (HPR) for Anti-Aging, Photodamage, and Acne
Hydroxypinacolone retinoate (HPR) has demonstrated positive effects as a topical anti-aging ingredient, the authors of the study writing, “Together these data suggest that HPR is an effective alternative to ATRA and other less potent retinoids in the treatment of aging skin without the detrimental side-effects. And the combination of retinoids and salicylic acid can be used to ameliorate the signs of photoaging.
Data have confirmed past studies indicating that topical retinoids are under-used for acne. Further, HPR has been successfully used to treat comedonal-papular, mild to moderate acne of the face. In this study, papain was also used, in addition to HPR, as an exfoliant, and in many cases acne patients may benefit from combination therapies, such as the use of retinoids (HPR) with salicylic acid to better treat acne.
Carotenoids, Like Beta-Carotene, Convert to Retinoids When Topically Applied
You’ll notice on the label of NeoGenesis Skin Restore Serum, that in addition to HPR, carotenoids, including beta-carotene, are included in the product. While topically applied carotenoids absorb into the skin and are converted to retinoids in the skin, the carotenoids also provide antioxidant benefit to the skin. The beautiful yellow color of the vitamin A product, Skin Restore Serum, reflects the yellow pigmented carotenoid antioxidants loaded into the serum.
The amount of carotenoids in the skin depends on dietary intake, and their bioavailability from various foods, with fruits and vegetables as an important source.. After absorption in the gut and transportation into the skin, carotenoids accumulate in the skin, including the adipocytes in the hypodermis. The skin protective benefits of carotenoids, especially from those residing in the epidermis, are many, including protection from UV and air pollution.
Retinoids and Photosensitivity
Photosensitivity to retinoids appears to be a rare event, and quite to the contrary, retinoids have been found to successfully treat some forms of skin photosensitivity. First, let’s dispel the somewhat common belief that topical retinoids enhance UV-induced inflammation. Smit et al (1999) evaluated the minimal erythema dose (MED) for UVB irradiation on topical all-trans RA (tretinoin cream 0.05%) pre-treated skin compared with vehicle cream pre-treated skin and untreated skin. Their study found no significant difference for the MED values either 24 or 48 h after UVB irradiation between the all-trans RA cream treated skin, and the vehicle cream treated skin and untreated skin. In other words, topical retinoid caused no enhanced inflammation when the skin is exposed to UV.
Second, Actinic folliculitis (AF) is a rare recurrent seasonal photodermatosis, relatively newly characterized by nonpruritic, monomorphic pustules and papules appearing 4-24 h after exposure to sunlight. Lesions usually affect the face but also appear on the upper chest and arms. Resolution normally occurs within 7-10 days with cessation of sunlight exposure. AF is resistant to standard treatments used for acne vulgaris and acne rosacea, with only oral retinoids previously being reported as effective. Academic dermatologists in the UK have reported that AF responding extremely effectively to a topical retinoid.
Discussing photosensitivity, be clear that HPA is relatively stable in light and in the air. Applying and using HPA in normal lighting conditions will not degrade the product.
Long Term andOveruse of Retinoids
While a significantly higher concentration of retinol (0.4%) is required to attain similar outcomes as observed with topical retinoic acid, retinol triggers similar histological alterations (epidermal thickening and dermal ECM production) as retinoic acid. However, inappropriate or excessive use of topical retinoids or retinoic acid may also result in potential side effects. These commonly include skin dryness, redness, and peeling, which can cause discomfort. However, these side effects typically diminish over time as the skin adjusts to the product. Evidence suggests that HPR will induce fewer adverse side-effects than the other retinoids.
Long-term use of retinoids (studied for up to 2 years) have found beneficial effects to the skin throughout the treatment period, and a good safety profile. While most of the benefit is seen within 6 months following onset of the treatment, long term use can maintain the positive effects.
Summary
Topical retinoids (TR) are a safe and effective addition to one’s skin care routine, especially for aged skin. TR provides major benefits to the skin, including increased thickness of the epidermis and dermis, and enhanced blood flow to the skin. There are few side effects of retinoids, and if chosen properly, retinoid products, such as those that use HPR, are well tolerated by those with sensitive skin. Photosensitivity is not an issue, and their use with vitamin C/antioxidant products, such as those using gentle liposomal vitamin C (liposomal ascorbic acid), provides extra benefit.
Adipose mesenchymal stem cells (ADSCs) have evolved to arise in the skin during the third trimester of fetal development. These cells arise just before birth so that they can be present following birth to tampen inflammation that may arise in the baby’s new hostile, non-sterile environment where the skin is under constant insult from injuries, toxins, UV, antigens, and pathogens.It’s why ADSCs and the molecules they release are preferred over, 1. bone marrow mesenchymal stem cells and platelets, which serve to induce inflammation and rapid fibrotic scarring, and 2. over umbilical cord mesenchymal stem cells, that have evolved to operate in the sterile conditions of the womb to form the cord, which is unlike skin structure and function, and since it’s a sterile environment, not dampen inflammation which is unneeded and doesn’t happen in the sterile environment where infection can’t happen.The molecules released from ADSCs are the safest and most effective stem cell released molecules to use as skin therapeutics.
Scientist think teleologically often. It’s one of the ways we reason through the discovery and invention of phenomenon. Teleology is relating to or involving the explanation of phenomena in terms of the purpose they serve rather than of the cause by which they arise. In other words, teleology or finality is a branch of causality giving the reason or an explanation for something as a function of its end, its purpose, or its goal, as opposed to as a function of its cause. Why is this thing present, what is it doing?
Adipose mesenchymal stem cells (ADSCs) have evolved to arise in the skin during the third trimester of fetal development and to be present throughout adult life. These cells arise just before birth. So the teleological questions are, why do they arise just before birth, and what are the doing in the adult skin during a person’s lifetime?
Teleologically thinking, the ADSCs are present following birth to tampen inflammation that may arise in the baby’s new hostile, non-sterile environment that presents after birth. The ADSCs arise as tissue specific stem cells in the skin that has developed during the third trimester. The stem cell niche of the skin will help to direct these ADSCs to develop in a manner that is tissue specific and serves to resolve inflammation in that adult skin. This sort of tissue specific development of the ADSCs doesn’t happen in the bone marrow or the umbilical cord, for example. Following birth, the skin is under constant insult from traumatic injuries, toxins, antigens, UV, and pathogens. Those are signals for inflammation. When the skin is compromised by these factors, evolution has given the skin an inflammatory response to fight associated infection. Any of these factors can lead to barrier disruption and an eventual infection, and the inflammatory response is the key to fighting infection. But inflammation is damaging. Not only does infection fight invading pathogens, inflammation also damages our own cells and tissues.
So inflammation has to be tampened, otherwise, if it is prolonged, necroinflammation ensues and our tissues become necrotic or otherwise damaged. Without inflammation being reduced, the damaging inflammatory pathways cause more inflammation and scale-up the damage. And what is present in adult skin to resolve inflammation? It’s the adipose mesenchymal stem cells (ADSCs) and the molecules that they release. In this case, the molecules from ADSCs can help the healing process by a number of mechanisms, including angiogenesis and reducing inflammation. The molecules from ADSCs induce an anti-inflammatory pro-regenerative state in the skin. Diabetic ulcers are example, where the necrotic tissue, such as Necrotizing fasciitis, has to be removed to reduce the inflammation. In these conditions, the ADSCs are no longer present at the site of open wound, and inflammation is hard to control. Addition of ADSC secretome facilitates the healing of the diabetic ulcer through a number of mechanisms, including the reduction of inflammation.
ADSCs are preferred over, 1. bone marrow mesenchymal stem cells and platelets, which serve to induce inflammation and rapid fibrotic scarring, and 2. over umbilical cord or placental mesenchymal stem cells, that have evolved to operate in the sterile conditions of the womb to form the cord, which is unlike skin structure and function, and since it’s a sterile environment, not dampen inflammation.
There’s much hype about cytokines from bone marrow mesenchymal stem cells. I’ve previously blogged about how bad these BMSC molecules are for the skin. Let’s quickly consider inflammation and the stem cells used by AnteAge to make their products: Bone Marrow Mesenchymal Stem Cells (BMSCs), and the molecules they release, prolong and enhance inflammation by increasing survival and function of neutrophils (Castella et al, 2011). Under hypoxic conditions, which induces the activation of TRL4, BMSCs secrete pro-inflammatory factors and decrease the polarization of macrophages from the M1 to M2 phenotype (Faulknor et al, 2017; Waterman et al, 2010). Therefore, BMSCs cultured in normal hypoxic conditions in the laboratory are secreting pro-inflammatory factors and when administered to wounded skin will induce inflammation by recruiting neutrophils and M1 type pro-inflammatory macrophages. When you put AnteAge on your skin, these are the pro-inflammatory molecules damaging your skin.
Safety and efficacy considerations: ADSCs preferred Over BMSCs
I’m asked frequently about the safety of using the molecules from ADSCs, so I’ll address it here. When addressing safety and efficacy concerns of stem cells, we must consider tissue-specific stem cells, first described by Dr. Elly Tanaka, a professor of science at the IMP in Vienna. Choosing the appropriate stem cell type to match the condition to be treated is critical not only to efficacy, but most importantly, safety of the therapeutic. Beyond the genetic and epigenetic factors that influence stem cell phenotype as embryonic stem cells differentiate into somatic stem cells, the immediate niche of the stem cell will have profound influence on the cell’s phenotype. If your wanting to regenerate skin, then use tissue specific stem cells from the skin. ADSCs and their secretome is efficacious and safe. Even ADSCs from cancer patients can been safely used for therapeutic purposes.
We don’t use umbilical cord mesenchymal stem cells (UMSCs) because they are not tissue specific to the skin, and they didn’t evolve to work in adult tissue where inflammation needs to be inhibited. Bone marrow mesenchymal stem cells (BMSCs) do appear in the skin, but only transiently in the skin during open wounds to close the wound quickly (yielding fibrotic scarring). induce inflammation (destructive to tissue), and cause high rates of proliferation (pro-oncogenic). If you think about it, the BMSCs appear transiently during an open wound to fight infection by inducing inflammation, and closing the open wound quickly by hyper-proliferation of cells. BMSCs and their released molecules didn’t evolve to be present in the skin for long periods of time – only transiently. Applying BMSC molecules for an extended time will induce too much inflammation and too much proliferation, leading to long term inflammation, fibrotic scarring, and a pro-oncogenic state.
Beyond their suboptimal efficacy profile, I’ll briefly explain some of the mechanisms underlying our choice of not using BMSCs because of a poor safety profile. The complexity of the bone marrow (BM) niche can lead to many stem cell phenotypes, whether we consider hematopoietic stem cells (HSCs) or bone marrow mesenchymal stem cells (BMSCs). Here I will discuss the properties of BMSCs, not HSCs. Because of the complexity, many BMSC phenotypes exist, including disease causing phenotypes that are varied and hard to distinguish – a part of the problem in using BMSC for therapeutic development. This complication, unlike that for ADSCS, includes recirculated cells, particularly recirculated cancer cells. Once a tumor cell disseminates into the BM, the cancer cell often displays phenotypic characteristics of BMSCs rendering cancer cells difficult to distinguish from BMSCs. BM is a site of BMSCs that may differentiate into HSCs [113] and recirculating blood cells that may differentiate into BMSCs [114,115]. BMSCs are also found outside of the niche in peripheral blood [116] and home into sites of injury [117] and cancer tissue where they are educated into becoming a pro-cancerous phenotype [118]. Recirculated melanoma and myelogenous leukemia cells [119] in BM interact with BMSCs to change the phenotype of the BMSC to one that is cancer promoting by enhancing their proliferation, migration, and invasion and altering the production of proteins involved in the regulation of the cell cycle [120]. Indeed, melanoma tumor cells start to disseminate to BM during the initial steps of tumor development [121]. In breast cancer patients, detection of recirculated cancer cells that disseminated in BM predicts recurrence of the cancer [122]. Cancer cells can fuse with BMSCs and change their phenotype [123], or release exosomes to change the phenotype of BMSCs to cancer promoting [124]. Indeed breast tumor cells fuse spontaneously with bone marrow mesenchymal stem cells [125]. This fusion may facilitate the exchange of cellular material from the cancer cell to the BMSC rendering the fused cell more oncogenic [126]. Further, others have found the same result of this fusion and exchange of cellular material, which has been found to increase metastasis. For example, Feng et al127,found that human hepatocellular carcinoma cells with a low metastatic potential exhibit a significantly increased metastatic potential following fusion with BMSCs in vitro and in xenograft studies. In the end, the BMSCs and their molecules/exosomes, having been conditioned by tumor cells, were found to increase the probability of cancer in human patients [128]. The various phenotypes of BMSCs, including the cancerous phenotypes are difficult to distinguish [36]. In contrast, even ADSCs derived from cancer patients have been found to be safe for therapeutic development [66].
One of many reasons why ADSCs are preferred compared to BMSCs is that ADSCs express a low level of major histocompatibility complex (MHC) class I molecules and do not express MHC class II and costimulatory molecules. Even the exosomes of BMSCs express MHC class II proteins [129]. These problems in BMSCs are amplified when using donor, allogeneic BMSCs that have been replicated many times, essentially aging the cells, during expansion to develop the therapeutic. This is in contradistinction to ADSCs. Critically, when comparing experimental data of BMSCs to ADSCs from the same human donor, “ADSCs have a “younger” phenotype,” according to stem cell scientists [130]. Indeed, Burrow et al found that BMSCs have, among other negative attributes compared to ADSCs, an increased level of senescence compared to matched ADSCs. Senescent cells develop the senescence-associated secretory phenotype (SASP), a pro-inflammatory set of molecules where the local tissue effects of a SASP or specific SASP components have been found to be involved in a wide variety of age-related pathologies in vivo such as hyperplastic diseases, including cancer [131]. Whereas the use of BMSC transplants has a history of medical adverse events, including the induction of cancer in the recipient (Maguire, 2019), fat grafting, along with its constituent ADSCs, have a long history of safety in medical procedures dating back to 1893 when the German surgeon Gustav Neuber transplanted adipose tissue from the arm to the orbit of the eye in an autologous procedure to fill the depressed space resulting from a postinfectious scar [132]. Fat grafting’s long history of being safe, regardless of the harvesting techniques used in patients [120,133], has been recently reviewed by physician-scientists at Baylor College of Medicine [134]. Furthermore, physician-scientists at Stanford University School of Medicine have recently reviewed the safety and efficacy of using ADSCs to augment the outcomes of autologous fat transfers [135]. 136,have found that ADSCs and fat grafting for treating breast cancer-related lymphedema is safe and efficacious during a one year follow-on, where patient-reported outcomes improved significantly with time. In a randomized, comparator-controlled, single-blind, parallel-group, multicenter study in which patients with diabetic foot ulcers were recruited consecutively from four centers, ADSCs in a hydrogel was compared to hydrogel control. Complete wound closure was achieved for 73% in the treatment group and 47% in the control group at week 8. Complete wound closure was achieved for 82% in the treatment group and 53% in the control group at week 12. The Kaplan–Meier (a non-parametric statistic used for small samples or for data without a normal distribution) median times to complete closure were 28.5 and 63.0 days for the treatment group and the control group, respectively [137]. Treatment of patients undergoing radiotherapy with adult ADSCs from lipoaspirate were followed for 31 months and patients with “otherwise untreatable patients exhibiting initial irreversible functional damage” were found to have systematic improvement or remission of symptoms in all of those evaluated [138]. In animal models with a full thickness skin wound, administration of ADSCs, either intravenously, intramuscularly, or topically, accelerates wound healing, with more rapid reepithelialization and increased granulation tissue formation [139], and topically applied the ADSCs improved skin wound healing by reducing inflammation through the induction of macrophage polarization from a pro-inflammatory (M1) to a pro-repair (M2) phenotype [140]. I’ve discussed some of the other mechanism by which ADSCs reduce inflammation in the skin in a recent blog.
Summary
Adipose mesenchymal stem cells (ADSCs), unlike stem cells from tissues other than the skin (BMSCs and UMSCs) and stem cells from non-adult sources in the womb (UMSCs), evolved to work in the skin of adults to inhibit inflammation and to reset the innate and adaptive immune systems of the skin to a anti-inflammatory, pro-regenerative healing state to maintain and regenerate normal, non-fibrotic skin structure and function.
The molecules released by adipose mesenchymal stem cells (ADSC) are known to bring skin cells out of senescence, and the mechanism of action is twofold: 1. the molecules released from ADSC contain SIRT1, and 2. the molecules released from ADSC increase SIRT1 expression in target cells. These are two of the many mechanisms of action underlying the ability of NeoGenesis‘ S2RM technology to rapidly and sustainably reverse and prevent the signs and symptoms of skin aging.
Longevity is a hot topic in the popular press, and the topic has now hit skincare. This is part of the “scientification” of skincare in the popular press that has arisen over the last few years. The trend has an upside and a downside. Learning about ingredients and how they work in the skin is important. The better informed we are, the better we can take care of our skin. The downside, is that non-scientists, including many practicing dermatologist, who have neither been trained as scientists, nor trained to analyze scientific studies, often proffer erroneous information about skin care in the popular press. For example, in my 2020 publication, in the section called “Example of Misinformation in Skin Care Marketing.” I describe how a practicing dermatologist in Miami makes many mistakes in describing skin care ingredients in her various popular press articles, including articles in a large newspaper.
Also, reading a Bloomberg article on what dermatologist think about anti-aging skin care products, I was once again shown an example of how misinformed are some practicing dermatologist. One dermatologist was saying not to use products that contain antimicrobial preservatives, but when looking at the products she has for sale on her website, guess what – many of the products she sells online contain an antimicrobial preservative. Looking at her blog, she talks a lot about using sunscreen – an important topic. But she misinforms the reader by saying that mineral sunscreens reflect light and UV. That’s incorrect because mineral sunscreens predominantly absorb the UV, not reflect it. I didn’t read anymore because I dislike misinformation – I’ll stick to reading informed articles from professors of dermatology, including scientists and physicians, who inform us based on scientific and clinical evidence.
Let’s look at what’s being said about longevity of the skin in the popular media, and have a brief look at some of the science in the scientific literature (PubMed, peer-reviewed journal articles).
Longevity in Skincare
As Jeannette Neumann in Bloomberg states:
In the same article, Neumann goes on to tell us that:
Key to the new product ate sirtuins. So what are sirtuins and what do they do? Sirtuins are a family of signaling proteins involved in metabolic regulation. They are ancient proteins in animal evolution and appear to possess a highly conserved molecular structure throughout all kingdoms of life. They are everywhere in lifeforms. And guess what the scientific evidence suggests: NeoGenesis not only has SIRT1 activators in our S2RM technology, but we also have the SIRT1 protein itself. We’ve had S2RM on the market for over 13 years as a topical product. It’s one of the reasons our products work so well.
Here’s a little more on sirtuins and how they’re activated. SIRT1 is a cellular defense protein that ensures survival by controlling metabolism when there is not enough energy supply to cells. SIRT1 is an important molecule in the control of redox states, apoptosis, and a number of life-extending mechanisms. By changing SIRT1 expression, a number of substances and factors can control the level of SIRT1 protein. Naturally occurring molecules that increase SIRT1 expression include, resveratrol, quercetin, fisetin, curcumin, and berberine. SIRT1 protein expression declines as a we age, and SIRT1 expression decreases with age in mice. SIRT1 has been referred to as a longevity-associated protein that could be used as a potential therapeutic target for extending human healthspan, and it is currently under investigation in the battle against cognitive decline, neurodegenerative diseases, and aging. SIRT1 has been reported to negatively regulate the expression of a number of inflammatory senescence-associated secretory phenotype (SASP) factors, including the SASP factor. SIRT1 produces neuronal protection in neurodegenerative disorders and memory impairment, and is crucial for synaptic plasticity and memory retention in neurons. Numerous studies have shown that p53 and p21 have a role in the control of the cell cycle, DNA repair, apoptosis, and other critical biological processes. Cell cycle arrest results from the activation of p53 and p21, which are responsible for replicative and stress-related senescence in cells. SIRT1 acts on p53 by deacetylating it, which negatively regulates p53’s transcriptional activity, essentially suppressing its function as a tumor suppressor and inhibiting apoptosis induced by stress or DNA damage. In other words, SIRT1 “dampens down” the activity of p53 by removing acetyl groups from it.
Senescent cells release a range of inflammatory proteins, such as SASP, which causes low-grade chronic inflammation and accelerates senescence. Loss of the key anti-aging molecule SIRT1 may be important for accelerating aging. Zhang et al (2023) found that aged mice displayed upregulation of senescence-related signals such p53 and p21 and downregulation of SIRT1 in the hippocampus. These abnormalities were reversed by the molecules released from mesenchymal stem cells (MSCs).
In our skin, fibroblasts are long-lived cells that are subject to much damage over the years. They can become senescent and pro-inflammatory. Studies have found that SIRT1 can protect human fibroblasts from senescence by promoting telomerase reverse transcriptase transcription (Yamashita et al, 2012). Further, Yuan et al (2012) found that SIRT1 improved the senescence of young MSCs during in vitro subculturing. In other words, SIRT1 protects young cells from stressors, such as oxidative stress, and keeps them healthy and from becoming pro-inflammatory senescent cell types.
As you can see from these studies, it’s not just about anti-aging, it’s about promoting longevity in the first place. We do both at NeoGenesis with our S2RM technology.
Failed company brings suboptimal skincare product to market by a manufacturer in Korea, known for fraudulent and corrupt stem cell science, even at it’s premier university, Seoul National University.
Benev is a company that couldn’t survive in the market, and had numerous problems as exemplified by this FDA review where they found poor quality control and the use of expired materials being used in production:
For example, Benev was using expired ingredients to manufacture drugs that went to market, and falsified documents to hide their egregious behavior (below is from a FDA Warning Letter to Benev):
“QCD” refers to Benev’s quality control department.
As a consequence of this violation, and may other violations, FDA concluded that Benev’s drug products were adulterated:
Resulting from continued poor performance, Benev sold themselves to a Korean company, ExoCoBio, that uses Benev to sell exosomes in the USA. A culture of corruption and fraud was highlighted by the veterinarian, Hwang Woo-suk, and his many conspirators who faked a landmark stem cell publication. That culture was exported to the USA by Benev. Previously, Benev worked with another local company called Invitrx, a company with a rich history of FDA violations, a long history, and led by a man, Habib Torfi, known for delivering stem cells to patients in a grocery bag.
There are numerous problems with what Benev (ExoCoBio) is doing to exosomes.
First, exosomes are only a fraction of what stem cells release, and without the non-exosomal fraction being combined with the exosomes, suboptimal results are achieved. In other words, when the exosomes aren’t isolated but are combined with the soluble fraction as is natural when the stem cells release their molecules, the results are superior to using only the isolated exosomes.
Second, they lyophilize their exosomes – this is a freeze-drying process that damages the molecules inside the exosome, and molecules attached to the outside of the exosome. Basically this harsh process removes all the water from the product, leaving a small amount of dry powder. The powder is full of damaged proteins and other molecules. Lyophilization leads to aggregation of proteins and their denaturization. “Unfortunately, the lyophilization process generates both freezing and drying stresses, which can denature proteins to various degrees” (Wang, 2000). Protein denaturation refers to the loss of biological activity through changes of the specific spatial conformation of protein in certain physical or chemical factors, resulting in the change of physical and chemical properties.
Lyophilization is used for the convenience of the company – it’s easier to store and ship a small pellet of lyophilized powder than it is to store and ship fresh, undamaged exosomes contained in their original solution.
From the Benev website we see they’re using lyophilized exosomes, and only the exosomes without the benefit of the soluble fraction (the overlapping text on their website is another example of the lack of attention to detail in this failed company):
To compare, NeoGenesis uses fresh (not damaged from freeze-drying) S2RM that contains both the 1. exosomal fraction, and 2. soluble fraction. Also, NeoGenesis uses both fractions from 3 cell types derived from the skin (mesenchymal stem cells and two types of fibroblasts). In contrast, Benev uses only a portion of the molecules released from one cell type, yielding a much depleted set of molecule types compared to NeoGenesis, many of which are damaged by Benev using lyophilization.
Another nearby company, Invitrx, in Lake Forest, is selling non-sterile exosomes for injection – allogenic injection. Talk about dangerous. Invitrx has a long history of unsafe practices. For example, illegally selling stem cells for injection, delivered in a paper grocery bag and selling non-sterile exosomes to physicians as exemplified in this FDA 486 Warning Letter, in which the agency details numerous non-sterile practices used to produce their exosomes.
You can read about the problems with lyophilization with many references to the published literature in my blog:
Wounding from procedures induces cellular replication, and replication may drive changes in cells and could push them toward a more tumorigenic state.“Tumors are wounds that don’t heal.”
Tissue specific stem and progenitor cells, such as the skin’s mesenchymal stem cells, fibroblasts, and keratinocytes, can persist during the lifetime or for extended periods of time in humans and contribute to both renewal and repair by giving rise to pools of progenitor cells that persist for various periods of time, replenish differentiated, i.e. mature cells, release many types of molecules involved in healing, and make short-term contribution to wound healing. Normally, these cell’s processes maintain and heal our skin throughout life. However, due to poor lifestyle, such as a diet that overfeeds us but under nourishes us, the nutrients needed to maintain proper function in these cells are lacking. Too much sun, leave-on products that are pro-inflammatory, and environmental exposures are other examples of lifestyle factors diminishing skin function. While hereditary and genetic factors may play a role, their contribution is minimal to developing diseases. Along with intrinsic aging, where our cells go through “wear and tear” to maintain themselves regardless of other impinging factors, what we do in life, i.e. our exposome is by far the most significant factor in maintaining health, including our skin health. Again, our exposome as a consequence of what we do in life, is the largest factor in our skin’s health. For example, if you don’t exercise, then the body won’t produce a normal complement of antioxidants. And, if you don’t eat a sufficient supply of fruits and vegetables, antioxidants will not be carried through the blood and pumped into the skin. And if you’ve induced chronic inflammation in the skin, perhaps through the continuous use of an inflammatory product or procedure, then the antioxidants and other nutrient may not be efficiently pumped from the blood supply into the skin. Yes, inflammation can interfere with the pumps in the blood vessels that bring nutrients from the blood supply into the skin.
As I have written, numerous studies have found that providing all the necessary nutrients, without an overabundance of calories, optimizes stem cell function in the body. Eating well also optimizes the cell function in cells other than stem cells, many of which act to support stem cell function. It’s all a tightly woven system, and the key here is to understand it’s a system. All of our cells work together. For example, even inflammation in the outer layers of the skin, the epidermis, leads to inflammation throughout the body. So what you do to your skin affects your whole body. If you’re using topical products that induce inflammation in the skin, you’re inducing inflammation in the body. If you’re having a procedure, such as laser, chemical peels or microneedling, you’re inducing inflammation in the skin and therefore inflammation in the body. As I have previously written, wounding the skin through the use of these procedures, induces not only inflammation, but proliferation too. This over-driving of cell proliferation leads to cellular exhaustion. Stem cell exhaustion or dysfunction increases with age, and especially with too many wounding procedures, and impedes the normal function of multiple tissues and systems. Dr. Leonard Hayflick, Ph.D., a professor at UCSF, discovered that cultured normal human cells have limited capacity to divide, after which they become senescent and can secrete inflammatory factors, a phenomenon now known as the ‘Hayflick limit’. Increase inflammation and/or increase proliferation, and you can drive cells towards their Hayflick Limit. That’s what too many wounding procedures can do to the skin. Further, chronic inflammation coupled with chronic proliferation of cells is a hallmark of cancer.
If you are having one of these wounding procedures, something that can induce prolonged inflammation, I recommend using a product, such as NeoGenesis Recovery, that quells inflammation. Here’s why I recommend Recovery: Stem cell released molecules from adult stem cells derived from the skin are the key ingredient in Recovery. These molecules, the so-called S2RM technology, powerfully quell inflammation and reset the immune system from one of inflammation to one of anti-inflammation and pro-repair. The results are dramatic, and inflammation is quickly reduced. And because healing is hastened, proliferation is reduced too. Too much proliferation of the cells in the skin can lead to cellular exhaustion, senescence, and aging of the tissue. So key to healthy skin, particularly while we’re aging, is to control inflammation and, importantly, control the damage to the skin. Too many procedures that wound the skin, will lead to eventual aging of the skin. Thus, one may see short term positive effects, but long term negative consequences.
So how does one induce modest amounts of cellular turnover to remediate skin problems such as lines and wrinkles, sagging, and discoloration? The key is evolutionary science. How does mother nature naturally keep the skin healthy and keep the cells turning-over at a safe rate? The key is feeding the skin: from the inside-out through diet, and from outside-in through topical application of carefully chosen products. And what you feed the skin is critical. There is no magic bullet, not one ingredient alone that will yield the desired results. Rather, the skin is a system, composed of many different elements, each element depending on its own set of needs. So to feed the skin, many different ingredients are needed. For example, Vitamin C is needed as an antioxidant and also to induce the production of collagen as well as to facilitate the post-translational modification of the collagen protein that has been produced. There are other functions of Vitamin C in the skin as well. Many other antioxidants are present in the skin, and they work synergistically. To optimize the antioxidant capacity of the skin, and not to have too much of one thing, many antioxidants need to be fed to the skin. Too much of one can have disastrous results. Consider Vitamin E. Tocopherol and its esters are some of the most well described antioxidants and they are commonly used for their ability to minimize ultraviolet damage. However, overuse of Vitamin E can inhibit glutathione-S-transferase, responsible for the removal of cytotoxic compounds related to tumorigenesis in the skin. And if too much Vitamin C is present, then oxidative oxygen radicals are formed through interactions with other molecules in the tissue. The consequences of this Vitamin C overload and the production of oxidants is yet to be adequately described.
The bottom line is to use a combination of ingredients that are natural to the skin, and not overload on a single or just a few ingredients. This is the scientifically-based strategy that I use when formulating products for NeoGenesis. I use Vitamin C in some of our products to help in the natural production of collagen turmover and to repair those collagen fibrils that will be present for years to come. Some collagen protein is called long-lived protein and will remain in the skin for decades. It can accumulate damage over the years, and one way to protect it and repair it is with the use of multiple types of antioxidants. Therefore, when I formulate products, Neogenesis offers multiple types of antioxidants that work synergistically. Sometimes people ask me, why do the Neogenesis products have different colors, and why aren’t they all white and creamy like other products on the market? The simple answer, our products have a multitude of ingredients that are important to the skin and have different colors. Think about your diet. If everything you ate was white, you die pretty quickly from malnutrition because you’re not eating all of those colorful fruits and vegetables that provide colorful nutrients to the body. All of these ingredients are necessary for the natural turnover and repair of your skin’s cells. Mother nature gives you a balance of nutrients, and that is what we do at NeoGenesis.
At Neogenesis we offer safe and natural, mostly skin-identical, ingredients that support the natural turnover of the skin’s cells. Skin identical ingredients include the S2RM that our skin’s stem cells make and ceramide and urea that are made by other cells. Skin identical ingredients also include ingredients that our bodies don’t make, but are brought into the skin through diet, including vitamin C and carrotenoids. We don’t give you a product loaded with just one ingredient at high amounts, such as EGF so that face reddens and puffs up like a water balloon, nor do we offer a lip product loaded with gobs of peppermint oil to irritate, cause an inflammatory immune reaction, and swell the lips so that everyone looks like they have Melkersson-Rosenthal syndrome. A core technology that we use at Neogenesis is our S2RM technology. As our skin ages or is compromised by poor health and poor diet, our stem cell function can decline. The molecules that we use at NeoGenesis are from stem cells in the skin that help to induce collagen production, protect collagen, and help to control the turnover of keratinocytes in the epidermis that are key to barrier formation. So what we’re doing at NeoGenesis is simply returning to the skin what was naturally present when we were young and healthy. In this way we restore natural cellular turnover and collagen production, without the adverse side effects of inflammation and over-proliferation associated with wounding procedures. And remember, if you do have a wounding procedure, be sure to use NeoGenesis Recovery before and after the procedure to minimize inflammation, normalize proliferation, and reset the innate and adaptive immune systems of the skin to a pro-healing mode. Please avoid certain stem cell products that are made with pro-inflammatory and pro-oncogenic bone marrow mesenchymal stem cell cytokines. With the use of Recovery, better results are realized from the procedure with fewer adverse side effects and less down time.